Meta Description:
How should metacarpal and phalangeal fractures be fixed? This article explains K-wire fixation, mini plate fixation, lag screw fixation, external fixation, surgical principles, rehabilitation, and functional recovery for hand fractures.
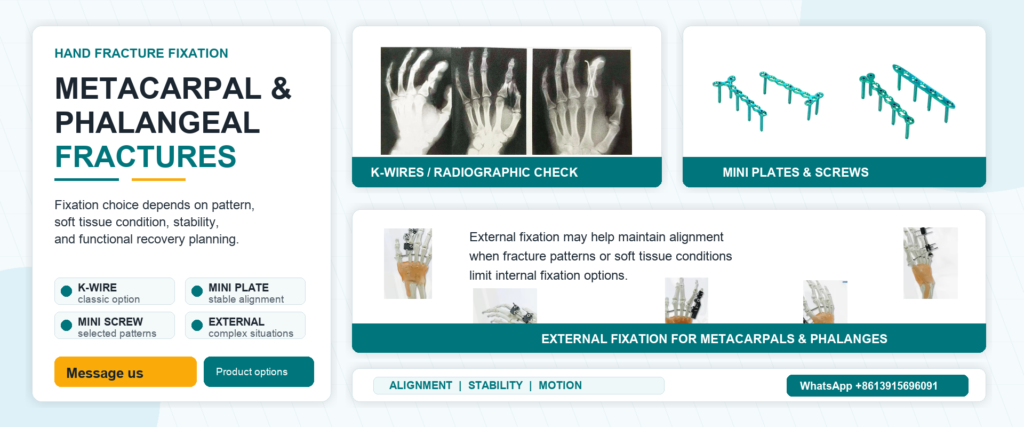
Metacarpal and phalangeal fracture fixation is never just about putting broken bones back together. The hand is not a simple long bone system. It is a precise machine built for grip, pinch, rotation, touch, and fine control. One small rotational deformity can make the fingers overlap during flexion. One ignored angulation can increase tendon friction and turn a “healed fracture” into a stiff, painful hand.
That is why the real goal is not only bone union. The real goal is accurate alignment, stable fixation, and early functional movement. If fixation is weak, rehabilitation becomes risky. If fixation is too bulky, the implant itself may block tendon gliding. This is the brutal truth of hand fracture treatment: the X-ray may look acceptable, but function decides whether the surgery actually worked.
The key principle in metacarpal and phalangeal fracture treatment is anatomical reduction with minimal but stable fixation. Rotation is the enemy. Mild shortening or angulation may sometimes be compensated by adjacent joints, especially in ring and little finger metacarpals. But rotational deformity does not forgive. When the patient flexes the fingers, the problem appears immediately: scissoring, overlap, deviation, and loss of precision.
Metacarpals generally tolerate shortening and dorsal angulation better than phalanges. However, this does not mean surgeons should accept poor reduction. Excessive palmar or dorsal angulation may destroy the smooth contact between bone and tendon, increase gliding resistance, and delay functional recovery. A good fixation strategy must support movement, not simply hold the bone in place. In hand surgery, TAM, TAF, grip strength, and tendon gliding matter as much as radiographic union.

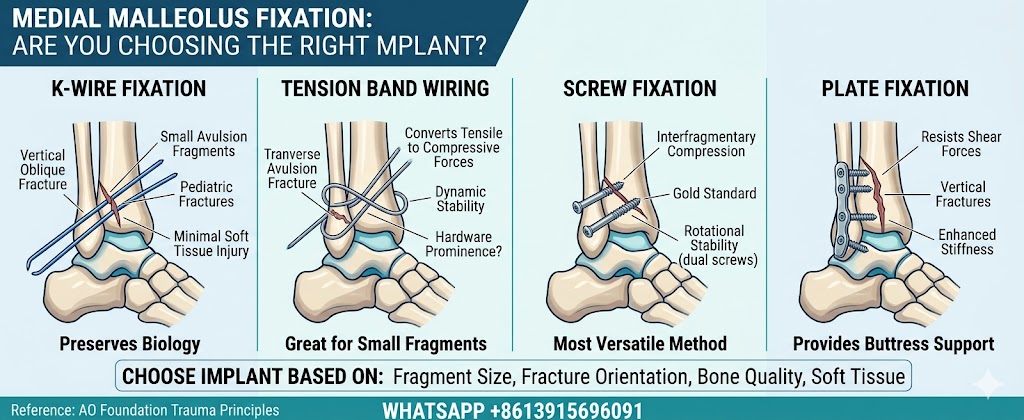
K-wire fixation for hand fractures has been used for decades and remains one of the most common fixation methods. It is simple, cost-effective, flexible, and causes less soft tissue stripping than open plate fixation. For intra-articular fractures, severe comminuted fractures, distal phalanx fractures, and small bone fragments, K-wires can still be extremely useful.
But K-wires have limits. A single K-wire usually cannot control rotation or shortening. Crossed K-wire fixation or multiple-wire fixation is often required. Traditional transarticular pinning may restrict joint motion and increase stiffness, although modern techniques under C-arm guidance can often avoid crossing joints.
Important points include:
- Avoid passing wires through tendons or extensor mechanisms.
- Use the fewest wires needed to achieve stability.
- Plan the entry point carefully before drilling.
- Avoid repeated attempts, which may further fragment the bone.
K-wires are not outdated. They are just unforgiving when used carelessly.
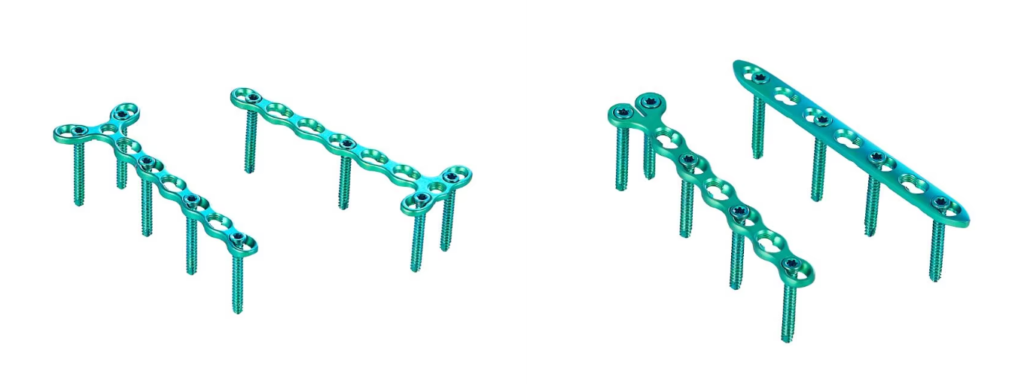
Mini plate fixation for metacarpal fractures provides stronger stability than K-wire fixation in many unstable patterns. It is especially valuable for unstable metacarpal shaft fractures, multiple metacarpal fractures, short oblique fractures, and cases requiring early active motion. A mini plate and screw system can better maintain length, alignment, and rotational control.
However, strength is not free. The hand has limited soft tissue space. In the proximal phalanx, middle phalanx, and periarticular regions, extensor tendons lie very close to the bone surface. A poorly placed plate can irritate tendons, limit gliding, cause adhesions, and sometimes require implant removal.
Mini plates are usually more suitable for metacarpal shaft fractures and selected proximal phalanx fractures. They should be placed dorsolaterally when possible to reduce tendon irritation. The goal is not to insert the strongest implant. The goal is to create stable fixation with the least biological damage.
Mini screw fixation for hand fractures can be an elegant option when the indication is correct. For long oblique or spiral fractures, lag screws can compress the fracture line, preserve more soft tissue than plate fixation, and reduce the need for extensive periosteal stripping. This makes mini screws attractive for surgeons who want stability without unnecessary implant bulk.
But the indication must be strict. For shaft fractures, the fracture line should usually be at least twice the diameter of the bone. For intra-articular avulsion fragments, the fragment must be large enough to safely hold the screw. If the bone fragment is too small, screw insertion may split it instead of fixing it.
Mini screws are not a universal replacement for plates or K-wires. They are a narrow, sharp tool. Used correctly, they can give compression, stability, and faster healing. Used badly, they fail fast.
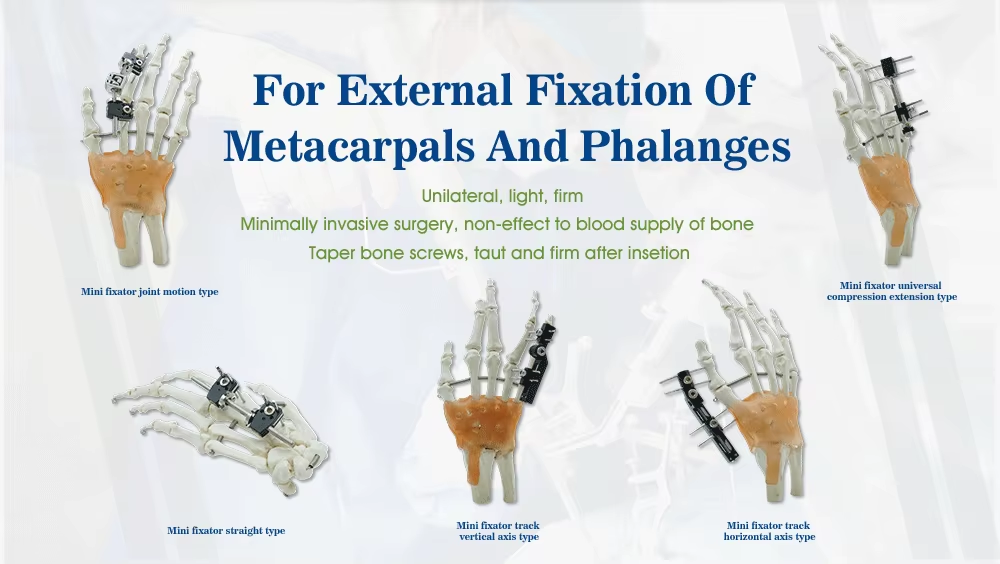
For severe comminuted fractures, open injuries, bone loss, or poor soft tissue conditions, external fixation for metacarpal and phalangeal fractures may be the smarter choice. When the bony framework is destroyed and internal fixation cannot reliably restore length, an external fixator can maintain alignment through traction and relative stability.
External fixation is especially useful in complex periarticular injuries and fractures where aggressive dissection would damage soft tissue. It can preserve length, allow wound care, and sometimes be combined with limited internal fixation.
Its drawbacks are also real: pin tract infection, pin loosening, stiffness when joints are bridged, and repeated X-ray exposure. External fixation should not be viewed as a “less advanced” method. In difficult fractures, it may be the most practical way to protect soft tissue while maintaining the skeletal frame.
Postoperative rehabilitation after hand fracture fixation is where the real outcome is decided. The most common complication after hand fractures is stiffness. Hematoma, prolonged immobilization, tendon adhesion, swelling, and capsular contracture can turn a technically successful fixation into a poor functional result.
Early controlled motion is essential, but only when fixation is stable enough. Mini plates and screws are often chosen because they allow earlier active movement. In contrast, patients treated with K-wire fixation usually require more caution during the first four weeks, especially with mechanical exercises.
Rehabilitation should focus on:
- Interphalangeal joint motion
- Flexor and extensor tendon gliding
- Swelling control
- Pain management
- Protection against fixation failure
For proximal phalanx fractures, this is even more critical because flexor and extensor tendons run very close to the bone. A few millimeters of tendon adhesion can seriously limit motion. This is where careless rehab loses the hand.
So, what is the best method for metacarpal and phalangeal fracture fixation? The honest answer is: it depends on the fracture pattern, location, soft tissue condition, stability demand, and rehabilitation plan. There is no single winner.
Unstable metacarpal fractures may benefit from mini plate fixation. Proximal phalanx fractures may require plates, screws, or K-wires depending on the location. Middle and distal phalanx fractures should be treated carefully, because bulky implants can disturb tendon gliding. Severe comminuted fractures may require external fixation combined with limited internal fixation.
For additional patient-level information, the American Academy of Orthopaedic Surgeons provides a useful overview here: AAOS OrthoInfo — Hand Fractures.
The final message is simple: hand fracture surgery is not about fixing bone alone. It is about preserving motion. Choose the wrong fixation method, and the fracture may heal—but the hand may still lose.