Meta Description:
Learn how the tibial intramedullary nailing approach affects alignment and anterior knee pain, including suprapatellar vs infrapatellar techniques, biomechanical insights, and surgical decision strategies.
Tibial Intramedullary Nailing Approach: Why Entry Point Determines Everything
Let’s be blunt.
Most complications in tibial nailing are not random.
They are predictable.
And they start with one decision:
👉 The tibial intramedullary nailing approach.
Choose the wrong entry point—and you don’t just miss alignment.
You create deformity.
In traditional practice, surgeons rely on infrapatellar approaches:
- transpatellar tendon
- medial parapatellar
They work well… for midshaft fractures.
But when you apply the same logic to proximal fractures?
That’s where things break down.
According to the AO Foundation, fracture fixation must align with mechanical axis and soft tissue balance.
Yet infrapatellar techniques often violate both.
👉 Result:
- valgus deformity
- anterior angulation
- unstable reduction
Understanding the tibial intramedullary nailing approach is not optional.
It’s the foundation of outcome.
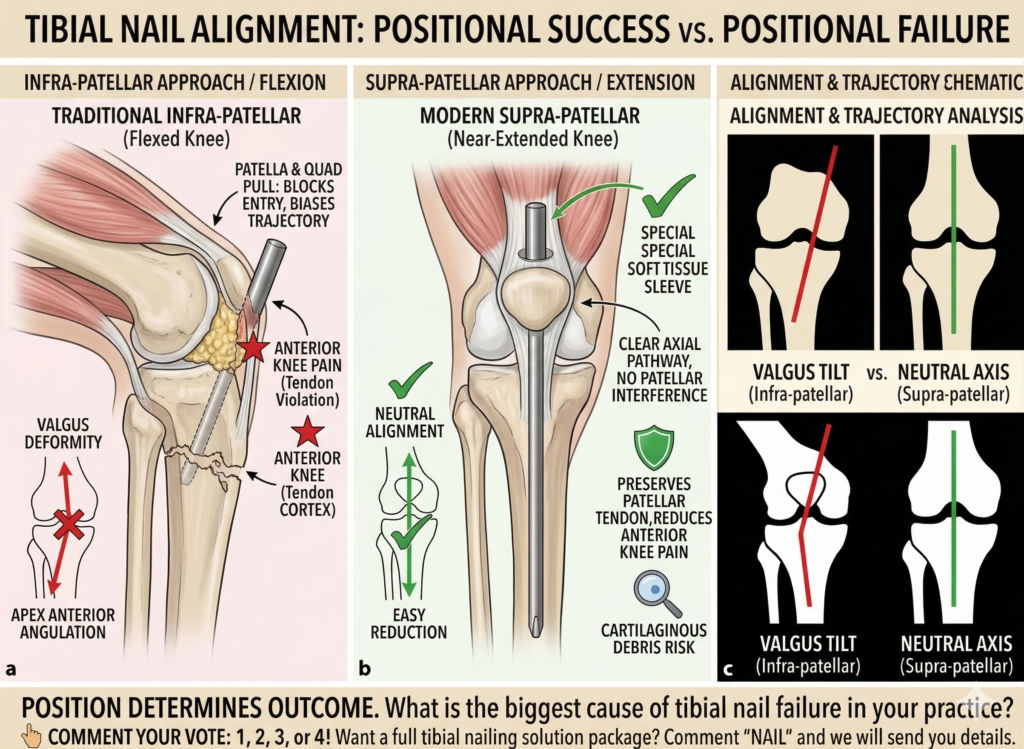
Why Proximal Tibial Fractures Fail with Traditional Approaches
Here’s the problem nobody likes to admit.
The tibial intramedullary nailing approach fails most often in proximal fractures.
Why?
Because the knee is flexed.
That changes everything.
Key deforming forces:
- Quadriceps tension → pulls proximal fragment anteriorly
- Patella blocking entry point → disrupts nail trajectory
- Mechanical conflict with posterior cortex → forces malalignment
What happens in reality:
- Nail insertion deviates from axis
- Proximal fragment tilts into valgus
- Sagittal plane alignment is lost
Even worse…
Using a medial parapatellar approach introduces another issue:
👉 Nail trajectory shifts medial → lateral, causing progressive valgus as it advances.
Add in anterior compartment tension—and the deformity becomes almost inevitable.
👉 This is exactly why tibial intramedullary nailing approach selection directly impacts alignment accuracy.
Suprapatellar Approach: Why It Changed the Game
Now let’s talk about what actually works.
The rise of the suprapatellar tibial intramedullary nailing approach is not a trend.
It’s a correction.
Instead of flexing the knee, the limb remains in a semi-extended position.
That single change eliminates multiple problems.
Key biomechanical advantages:
- Reduced quadriceps tension
- Straight-line nail insertion
- Better alignment with tibial axis
- Less posterior cortex conflict
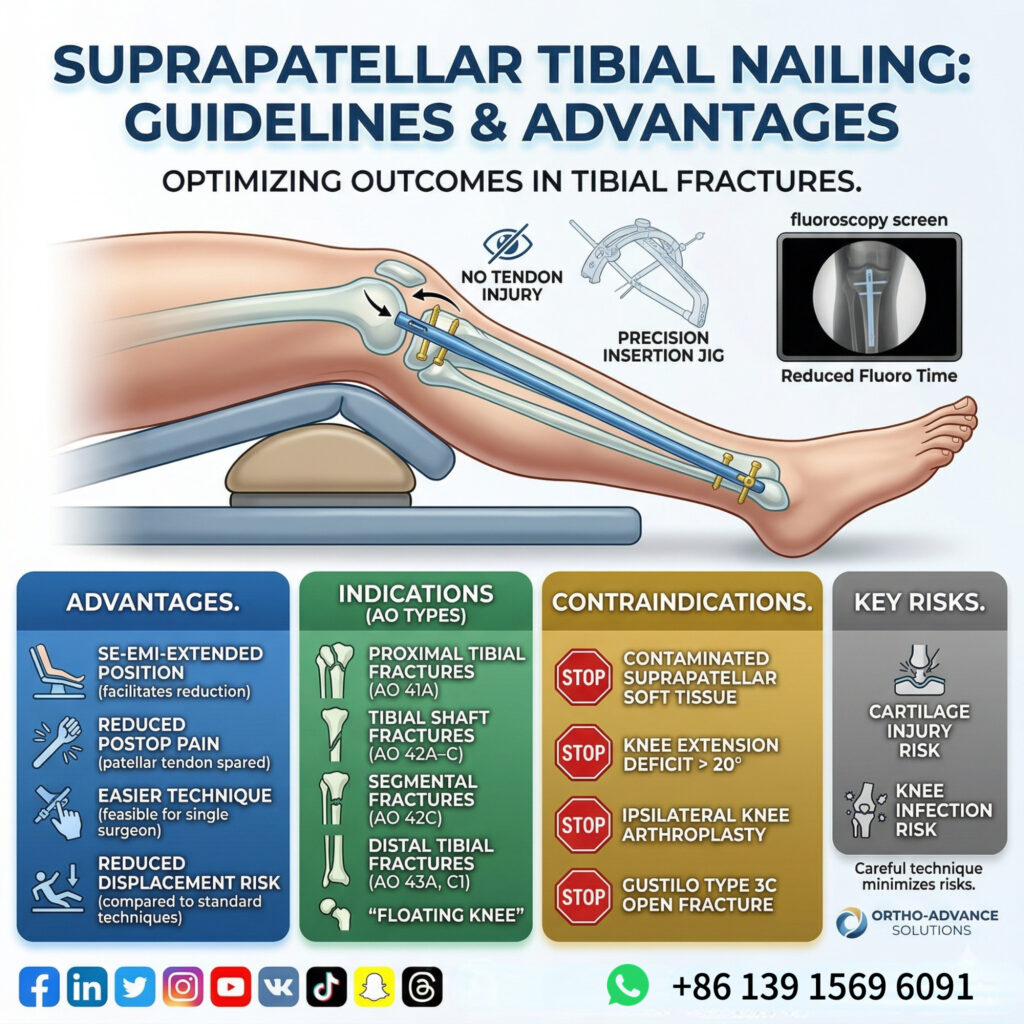
Clinical benefits:
✔ Easier fracture reduction
✔ More stable alignment during insertion
✔ Shorter fluoroscopy time
✔ Improved reproducibility
Studies show fluoroscopy time is significantly reduced compared to infrapatellar techniques.
👉 Translation:
The suprapatellar tibial intramedullary nailing approach aligns mechanics with anatomy.
That’s why it works.
Anterior Knee Pain: The Hidden Cost of Your Approach
Here’s a statistic that should make you uncomfortable:
👉 50–70% of patients experience anterior knee pain after tibial nailing.
And yet…
Many surgeons still underestimate the role of the tibial intramedullary nailing approach.
Main causes of pain:
- Patellar tendon injury
- Hoffa fat pad scarring
- Injury to infrapatellar branch of saphenous nerve
- Surgical scar sensitivity
Why suprapatellar reduces pain:
- No direct patellar tendon violation
- Avoids infrapatellar nerve injury
- Preserves anterior knee soft tissue
Instead, the nail passes through the quadriceps tendon, leaving the patellar tendon intact.
👉 Result:
- Lower incidence of anterior knee pain
- Less postoperative numbness
- Better functional recovery
Reality check:
Not all pain disappears.
But the difference is clinically meaningful.
And it starts with the tibial intramedullary nailing approach.
Limitations of the Suprapatellar Approach: What You Must Not Ignore
Let’s stay objective.
The suprapatellar tibial intramedullary nailing approach is not perfect.
Potential concerns:
- Risk of intra-articular cartilage injury
- Reaming debris entering knee joint
- Possible infection risk
Clinical reality:
Experience from retrograde femoral nailing suggests these risks are lower than initially feared.
No strong evidence shows long-term joint damage when proper technique is used.
Another practical issue:
👉 Implant removal
While removal through the suprapatellar route is possible…
Most surgeons still prefer infrapatellar removal due to technical simplicity.
👉 Bottom line:
This approach is powerful—but demands precision.
Decision Framework: Choosing the Right Tibial Intramedullary Nailing Approach
Let’s simplify everything.
✅ Use suprapatellar approach when:
- Proximal tibial fractures
- Segmental fractures
- Difficult alignment cases
- Need for reduced fluoroscopy time
⚠️ Consider infrapatellar approach when:
- Surgeon experience is limited
- Concern about intra-articular violation
- Planned implant removal strategy
👉 The rule:
Choose the tibial intramedullary nailing approach that protects alignment first—and soft tissue second.
Not the one you’re most comfortable with.
Final Thought: Alignment Is Not Luck—It’s Strategy
Tibial nailing failures are rarely accidents.
They are decisions.
And most of them trace back to one thing:
👉 The tibial intramedullary nailing approach.
Change the approach…
And you change the outcome.
More info.