Meta Description:
Explore external fixator vs internal fixation in trauma surgery. Learn when external fixation offers faster, safer stabilization and why surgeons are rethinking traditional internal fixation strategies.
The Hidden Debate Behind External Fixator vs Internal Fixation
Let’s be honest.
In modern orthopedic trauma care, internal fixation—plates and intramedullary nails—has become the default choice. It’s familiar. It’s widely taught. It feels definitive.
But here’s the uncomfortable truth:
External fixator vs internal fixation is not a solved debate.
In fact, many experienced trauma surgeons quietly acknowledge that internal fixation is not always the best option—especially in high-risk cases.
Why?
Because trauma is messy.
Soft tissue damage.
Open wounds.
Hemodynamic instability.
In these scenarios, rushing into internal fixation can increase complications.
According to the AO Foundation, fracture management must balance mechanical stability with biological preservation. That balance is exactly where external fixation shines.
Understanding external fixator vs internal fixation means recognizing that the “best” solution depends on the situation—not tradition.
When External Fixation Becomes the Smarter Choice
External fixation is often underestimated.
But in reality, it solves problems that internal implants sometimes cannot.
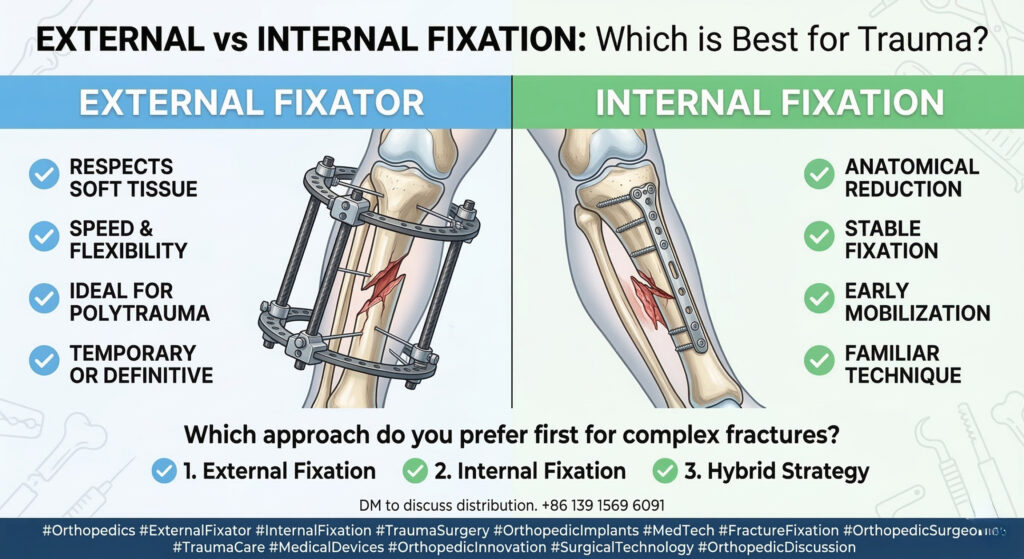
When evaluating external fixator vs internal fixation, certain clinical scenarios clearly favor external fixation:
- Severe soft tissue injury where surgical exposure risks further damage
- Open fractures requiring staged management
- Polytrauma patients needing rapid stabilization
- Damage control orthopedics (DCO) situations
External fixation offers three critical advantages:
- Speed – fast application in emergency settings
- Flexibility – easy adjustment without reopening the fracture site
- Biological preservation – minimal disruption to soft tissue and blood supply
These benefits are not theoretical. They directly impact patient survival and recovery.
This is why, in the debate of external fixator vs internal fixation, external systems remain indispensable.
Why Internal Fixation Still Dominates — And Its Limitations
Despite these advantages, internal fixation continues to dominate orthopedic practice.
Why?
Because it delivers:
- Stable anatomical reduction
- Early mobilization
- Familiar surgical workflows
However, when analyzing external fixator vs internal fixation, we must also acknowledge the limitations of internal methods.
Internal fixation can:
- Require extensive soft tissue dissection
- Increase infection risk in contaminated wounds
- Delay surgery in unstable patients
In complex trauma, these factors can become critical.
Sometimes, the problem is not the implant itself—but the timing and context of its use.
Surgeons may default to internal fixation because it is routine.
But routine is not always optimal.
The Evolution of Modern External Fixation Systems
One reason external fixation has been overlooked is its outdated image.
Bulky frames.
Heavy components.
Complicated assembly.
But that perception is changing rapidly.
Modern systems are redefining external fixator vs internal fixation by introducing advanced features:
- Radiolucent carbon fiber rods for improved imaging
- Lightweight modular clamps for better handling
- Snap-fit assembly systems for faster surgical setup
- Adaptable configurations for complex fracture patterns
These innovations transform external fixation from a temporary solution into a powerful, strategic tool.
The gap between external and internal fixation is narrowing—and in some cases, reversing.
The Real Future: External Fixator vs Internal Fixation Is the Wrong Question
Here’s the bigger insight.
The future of trauma surgery is not about choosing sides.
It’s about choosing wisely.
The real answer to external fixator vs internal fixation is not either/or.
It’s when and how.
A hybrid strategy is often the most effective approach:
- External fixation for immediate stabilization
- Internal fixation for definitive treatment
This staged approach minimizes risk while optimizing outcomes.
Surgeons who master this decision-making process gain a significant advantage.
Because trauma surgery is not about tools.
It’s about timing, judgment, and adaptability.
A Question for the Orthopedic Community
So let’s ask the real question.
Are we always choosing internal fixation because it’s better?
Or because it’s familiar?
💬 For complex fractures, what is your preferred first approach?
1️⃣ External fixation
2️⃣ Internal fixation
3️⃣ Hybrid strategy
Comment your answer below.
Orthopedics #ExternalFixator #InternalFixation #TraumaSurgery #OrthopedicImplants #FractureFixation #OrthopedicInnovation #MedicalDevices #SurgicalTechnology #TraumaCare
Like and share, your hands will be left with the fragrance!