Soft tissue foreign bodies or wounds associated with foreign bodies result from blunt/abrasive trauma or penetrating trauma. Patients may present early or late with a plethora of symptoms and signs. The foreign bodies can be divided into three groups according to their composition: (a) metallic, (b) organic, and (c) inorganic. This activity reviews the indications, procedure, and associated complications and the role of the interprofessional team in the care of this condition.
Objectives:
- Identify the indications for foreign body removal.
- Describe the technique in regards to foreign body removal.
- Review appropriate evaluation of the potential complications of foreign body removal.
- Summarize interprofessional team strategies for improving care coordination and communication to advance foreign body removal and improve outcomes.
Introduction
Soft tissue foreign bodies or wounds associated with foreign bodies are caused by blunt, abrasive, or penetrating trauma. Patients may present early or late with a plethora of symptoms and signs. Soft tissue foreign bodies or wounds associated with foreign bodies result from blunt/abrasive trauma or penetrating trauma. Patients may present early or late with a plethora of symptoms and signs. The foreign bodies can be divided into three groups according to their composition: (a) metallic, (b) organic, and (c) inorganic.
They are extremely common and varied. Some require removal in the theatre, whereas some are removable in the emergency department. Knowing how, but also when and when not to remove foreign bodies, is key.
Anatomy and Physiology
The anatomy involved is highly variable, depending on the position and depth of the wound and foreign body. However, the same principles need to be applied. Firstly, know the anatomy of where you are operating. This seems obvious, but it will guide us toward the potential complications and difficulties encountered.
Neurovascular structures will be the main concern. They can either be damaged at the point of injury or at risk of iatrogenic damage through surgical exploration. Being aware of all other structures is also paramount. With any potential surrounding structure being damaged means, these may need primary repair. This, in turn, may require a different specialist to be available; this should be considered when planning any procedure.
Indications
An absolute indication for exploration and attempted removal of a foreign body is any patient presenting with neurovascular compromise or infection. Ongoing pain, functional impairment, and the sensation of foreign material a strong indications for surgery. Weaker indications are patient requests and cosmetic deformity.[1]
Contraindications
Patients who may not require exploration and removal of foreign bodies are in clean wounds with no evidence of infection, no awareness of the foreign body, and where it is likely to be more traumatic to locate and remove the foreign body.[2][3]There is scope for delayed removal if the patient were to become aware of their foreign body or develop a complication.
Equipment
The equipment needed is normally quite standard but is by surgeon preference — a scalpel of varying sizes, a minor orthopedic set, which contains a variety of instruments. Needles of varying sizes can be beneficial for triangulation. An ultrasound machine or image intensifier is used for intraoperative identification (foreign body material dependent). Also needed are sutures for closure and a variation of dressings. For smaller foreign bodies, surgeons may request magnification loupes.
Personnel人员
Foremost a surgeon with an adequate skill level for exploration and removal is required. An anesthetic operating department practitioner (ODP), surgical scrub nurse, and an un-scrubbed member of the surgical team are needed. If the procedure is not being performed under a local anesthetic, then an anesthetist will be required for a general or regional anesthetic. If performed in the emergency department, the surgeon may have to rely on a junior surgical colleague for support and assistance.
Preparation
Antibiotics
In a clean, non-contaminated wound, there is no evidence to suggest antibiotics are required.[4]In any dirty or contaminated wound, antibiotics should be used by the hospital policy or in conjunction with the hospital microbiologist. Depending on the foreign body, it is prudent to find out the patient’s tetanus status and act accordingly.
Anesthetic
For superficial and extremity wounds, there is the potential for local anesthetic infiltration. If this is not possible or the clinician believes that more extensive washout and exploration is necessary, then a general or regional anesthetic is required.
Positioning
With the wide variety of possible wounds, this should be dynamic, as it will be wound/patient-specific. It should allow for adequate exposure and surgeon comfort while operating.
Further Considerations
Limb tourniquets may be required. It would not be recommended to use exsanguination as this could displace the foreign body, simple elevation should suffice.
Technique or Treatment
The patient is positioned per the surgeon’s preference. They are then prepped and draped with an appropriate antiseptic. As mentioned, if using a tourniquet, the limb should be elevated before it is inflated, this is to reduce the risk of exsanguination dislodging or moving the foreign body. If using an imaging modality intraoperatively (ultrasound/image intensifier), have this readily available and sterile at the beginning of the procedure.
Direct
If going through the current wound, it will likely need to be extended to improve exposure. Any contaminated wounds need thorough irrigation with sterile saline. Sometimes simple exploration will be enough to find and remove the foreign body. If this is the case, and the wound is clean, it can be closed with interrupted non-absorbable sutures. If infected, it will need to be left open and reviewed following local policy, normally 48 hours, and the aim of healing via secondary intention.
Indirect
In chronic foreign bodies, without wounds, deciding on the approach can be more difficult. As the foreign body is likely to have moved, going through the area of original injury may not be helpful. This is where the use of ultrasound or an image intensifier can be beneficial. Ultrasound can be used for initial incision, whereas image intensifiers can be better for triangulation. Using an artery clip, have them open with the tips around the foreign body in two views (anteroposterior and lateral) the clip can then be closed (hopefully around the foreign body) and the foreign body removed. Another novel method is using the image intensifier and a straight metal object in the foreign body’s longitudinal axis to guide an incision and then similarly use a clip as described above.[5]
A novel technique of vacuum-assisted foreign body extraction technique using a syringe has recently been described.[6]
Complications
The first complication of concern is neurovascular damage, either iatrogenic, during surgery, or directly from the patient’s injury. Depending on the extent of the damage would then indicate if any further intervention was required.
With any operation, infection is a risk; this is particularly relevant with foreign material and a penetrating injury. Although copious lavage is used, an infection can still occur. This may be treated with a course of antibiotics; however, it may also require further debridement in theatre.[7]There is a risk of local infection including osteomyelitis from a retained foreign body.[8]
Unfortunately, some foreign bodies are extremely small and can be very difficult to find on exploration, even if using loupes; thus, one final complication is a failure to remove foreign bodies. Sometimes the decision needs to be made to stop exploration for the objects if it is going to be more damaging. This can usually be done safely with ongoing observation and treated expectantly.[9]
With all these complications, the patient should have been counseled at the time of injury or before surgery so that adequate consent is obtainable.
Clinical Significance
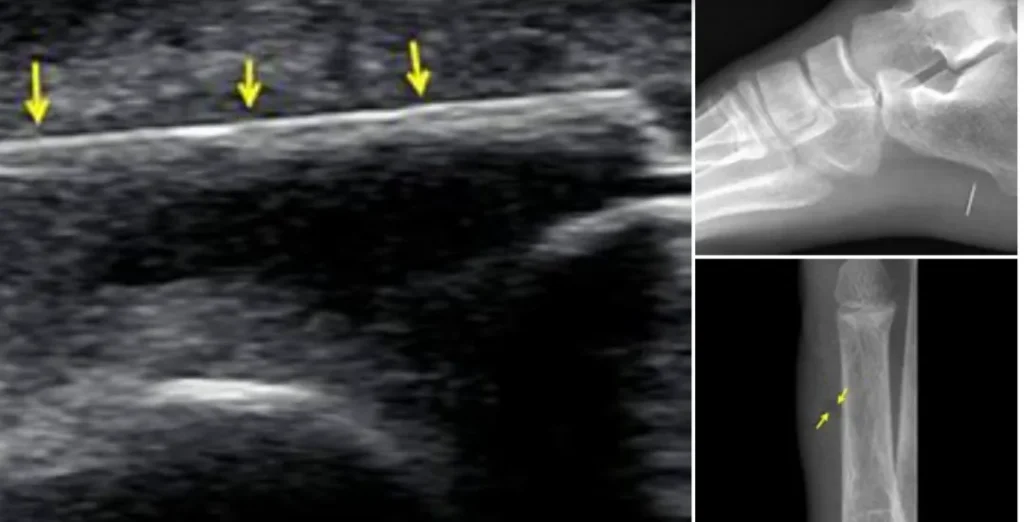
Metallic foreign bodies have a high atomic number and hence are readily visible on plain radiographs. The organic ones are those of vegetative origin like wood splinters or thorns. Inorganic materials are non-living beings like glass, plastic, or rubber. If an organic foreign body is suspected, it may be difficult to identify it on radiographs. As a result, the clinician needs to be extra diligent in wound exploration and inform the patient to return immediately if any signs of infection or foreign body develop. The organic foreign bodies are identifiable using ultrasound pre or intraoperatively. If identified preoperatively, they can also be marked to aid in their removal, and this is particularly beneficial in chronic foreign bodies where a wound is no longer present. The inorganic materials can be visible on radiographs or ultrasound, but this is variable. Usually, the glass will be visible on a plain radiograph. For deeper foreign bodies when there is concern about their involvement with specific structures, computed tomography may be required for better visualization.[10] In cases where contamination is suspected or confirmed, the patient should be taken to the operating room for extensive wound lavage and exploration.[11][12]
The ideal timefor foreign body removal is the first 24 hours after an injury to allow better evaluation of the entry and exit sites of the wound and to minimize the inflammatory response and scar formation.[1]
Enhancing Healthcare Team Outcomes
Foreign bodies are common but extremely varied. They range from being very difficult and very easy to remove – this means that they do not all require a trip to the operating theatre for their removal. For the easier foreign bodies, they are removable in the emergency department; however, there needs to be adequate support from surgical specialties to get involved for more complicated retrievals.
The key to enhancing outcomes is good communication with the patient. Not only when explaining all the complications and risks, but also that not all foreign bodies require removal.[9]Trying to dissuade patients from surgery that have been previously told they need can be psychologically detrimental. Finally, not leaving the task of surgical removal to an inexperienced and unsupervised surgeon, as ‘straight forward’ foreign body removals, can still become difficult.