Meta Description:
Discover when to use suprapatellar intramedullary nailing, including indications, advantages, risks, and contraindications. Learn how this technique improves tibial fracture outcomes.
When Should You Use Suprapatellar Intramedullary Nailing—And Why Many Surgeons Still Hesitate
Let’s be honest.
The debate around when to use suprapatellar intramedullary nailing is not about technique.
It’s about mindset.
For years, surgeons were trained in the infrapatellar approach. It became habit. Comfortable. Predictable.
But comfort is not always optimal.
The reality? Many complex tibial fractures are still treated with suboptimal alignment because surgeons hesitate to switch approaches.
According to the AO Foundation, alignment control and soft tissue preservation are critical for fracture healing. Yet traditional techniques often compromise both.
So here’s the question:
👉 Are we choosing techniques based on outcomes?
👉 Or based on what we’re used to?
Understanding when to use suprapatellar intramedullary nailing means breaking that habit.
Core Indications: When to Use Suprapatellar Intramedullary Nailing in Real Practice
If you want a clear answer to when to use suprapatellar intramedullary nailing, start here.
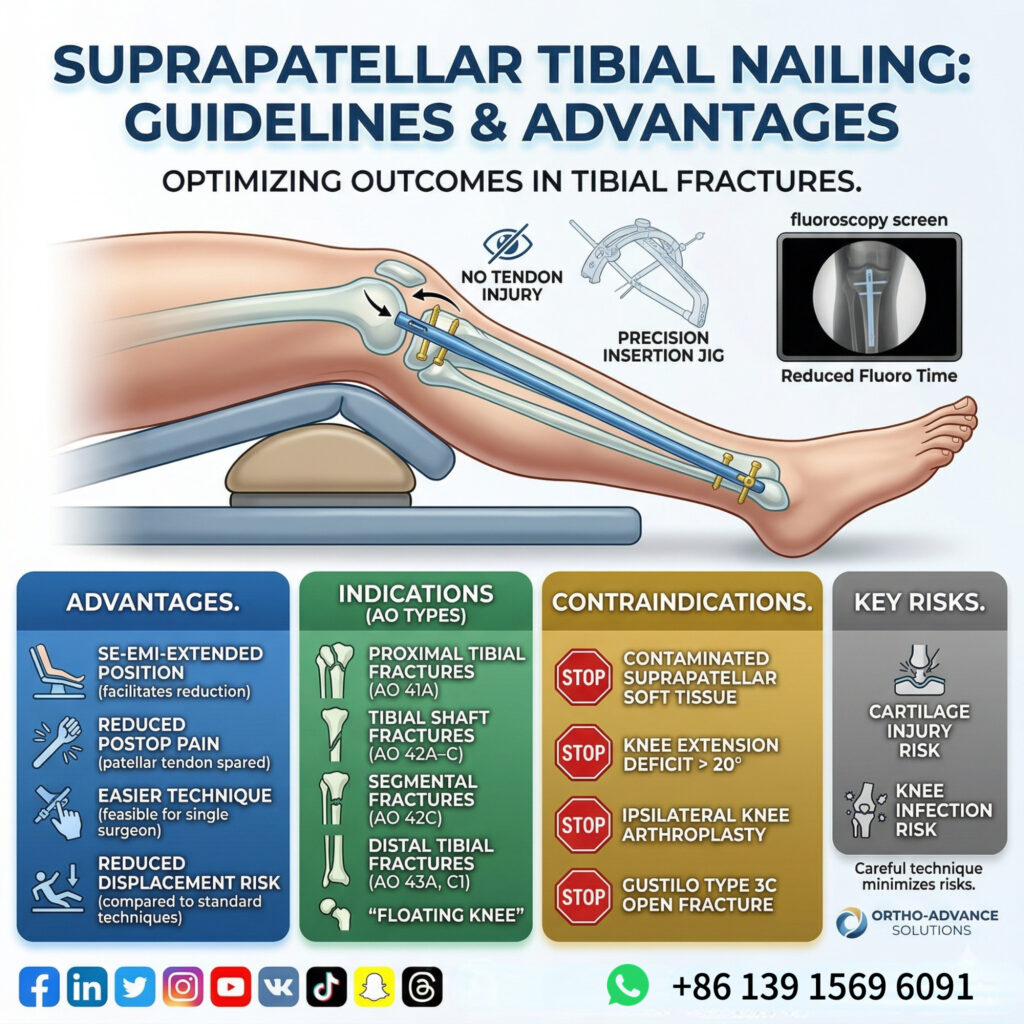
🔥 Ideal indications include:
- Proximal tibial extra-articular fractures (AO 41A)
- Tibial shaft fractures (AO 42A–C)
- Segmental tibial fractures (AO 42C)
- Distal tibial fractures (AO 43A & C1)
- Floating knee injuries
These are not random.
They share one common problem:
👉 High risk of malalignment with traditional infrapatellar techniques
Why suprapatellar works better here:
- Semi-extended knee position reduces deforming forces
- Easier fracture reduction and maintenance
- More accurate mechanical alignment
👉 Translation:
When to use suprapatellar intramedullary nailing = when alignment matters most.
Biomechanical Advantage: Why This Technique Changes Outcomes
Understanding when to use suprapatellar intramedullary nailing requires looking beyond indications.
It’s about physics.
Traditional infrapatellar nailing forces the knee into flexion. That creates:
- Quadriceps tension
- Anterior deforming forces
- Difficulty maintaining reduction
Suprapatellar nailing flips this.
Key advantages:
- Semi-extended positioning → muscle relaxation
- Improved control of proximal fragments
- Reduced risk of sagittal plane deformity
Clinical benefits include:
✔ Lower malalignment rates in proximal fractures
✔ Easier nail insertion trajectory
✔ Reduced need for repeated manipulation
✔ Shorter fluoroscopy time
👉 In complex cases, this is not a small improvement.
It’s the difference between acceptable and optimal.
Hidden Advantages: What Surgeons Often Underestimate
Most discussions about when to use suprapatellar intramedullary nailing focus on alignment.
But that’s only half the story.
Underrated benefits:
- Single-surgeon feasibility
- Better workflow in polytrauma settings
- Easier positioning in multi-team surgery
- Less dependency on assistants
Patient-centered advantages:
- Lower incidence of anterior knee pain
- No direct damage to the patellar tendon
- Improved early postoperative comfort
👉 In high-volume trauma centers, these advantages compound.
Efficiency improves. Fatigue decreases. Outcomes stabilize.
And yet… many surgeons still hesitate.
Risks and Limitations: When NOT to Use Suprapatellar Intramedullary Nailing
Let’s cut through the hype.
Knowing when to use suprapatellar intramedullary nailing also means knowing when to avoid it.
❌ Absolute or strong contraindications:
- Severe soft tissue damage or infection in suprapatellar region
- Contaminated wounds involving the entry pathway
⚠️ Relative contraindications:
- Gustilo type III C open fractures
- Ipsilateral knee prosthesis
- Knee fusion
- Limited knee extension (>20° deficit)
- Tibial plateau fractures involving entry point
- Existing implants blocking entry
Key risks:
- Potential cartilage damage
- Increased risk of intra-articular contamination
- Implant removal may require different approach
👉 Bottom line:
This is not a universal solution.
It’s a precision tool.
Decision Framework: When to Use Suprapatellar Intramedullary Nailing Step-by-Step
Let’s simplify the decision.
✅ Choose suprapatellar approach when:
- Proximal or distal tibial fractures
- Segmental or comminuted fractures
- Polytrauma or floating knee
- Need for faster, more stable reduction
❌ Avoid or reconsider when:
- Severe contamination
- Poor suprapatellar soft tissue condition
- Knee joint pathology or implants
- Entry point compromised
👉 The rule is simple:
Use suprapatellar intramedullary nailing when stability + alignment + efficiency matter more than tradition.
Final Thought: This Is Not a Technique Shift—It’s a Mindset Shift
The real question is not:
👉 “When to use suprapatellar intramedullary nailing?”
The real question is:
👉 “Are you willing to abandon outdated habits?”
Because modern trauma surgery is not about doing what’s familiar.
It’s about doing what works.
And in many complex tibial fractures…
The answer is already clear.
More info.