Metacarpal fractures account for 60% of hand fractures. Direct violent injuries can lead to transverse metacarpal fractures, while indirect and torsional violence often lead to spiral or comminuted fractures. Most metacarpal fractures can be treated with closed reduction and plaster fixation. For patients with angulation > 30°, rotation > 5°, shortening > 5mm and difficulty in closed reduction, surgical treatment is recommended to avoid finger dysfunction. Due to the obstruction of the adjacent metacarpal bones and the thick soft tissue on the palm side, closed reduction and maintenance of reduction of the fourth metacarpal fracture are more difficult, and surgical treatment is more common.

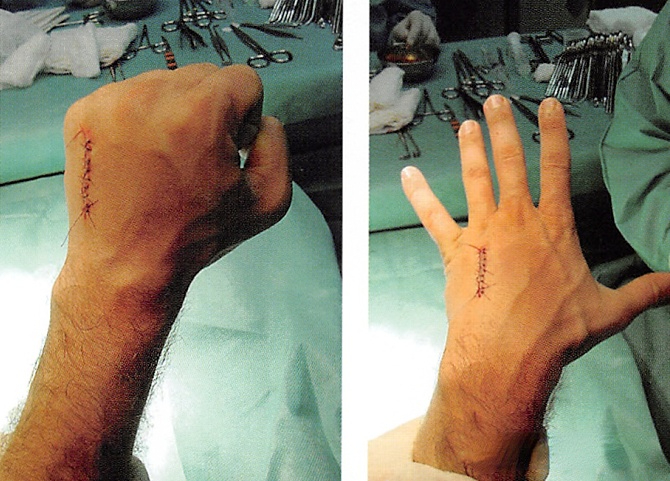
Dorsal plate and screw internal fixation can provide accurate fixation and is simple to operate, but it leaves a large surgical scar and requires secondary removal of the internal fixation.
In recent years, closed reduction and Kirschner wire fixation has the advantages of minimally invasive surgery and no need for secondary surgery, making it more and more widely used in metacarpal and phalangeal fractures. Scholars from Hebei Third Hospital published an article describing a method of closed reduction and Kirschner wire fixation of the fourth metacarpal fracture for your reference:

Surgical procedures
Step 1: Routine disinfection and draping, ulnar nerve block anesthesia. Metacarpal fractures are usually displaced distally, and the proximal part is relatively fixed due to the presence of the carpometacarpal joint and adjacent metacarpal bones. First, a 1.5mm Kirschner wire is inserted through the 5th metacarpal bone into the proximal part of the 4th metacarpal fracture to fix the proximal part of the fracture.

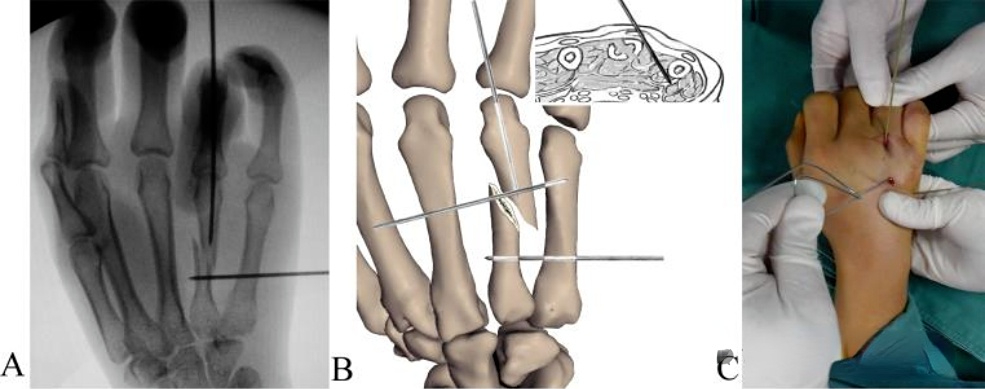
Step 2: Flex the metacarpophalangeal joint 90°, insert a 1.5mm Kirschner wire through the distal articular surface of the metacarpal bone and penetrate into the distal bone marrow. Then traction the ring finger and close the fracture ends of the compression fracture. If reduction is difficult, the Kirschner wire can be used to pry through the skin or bend the Kirschner wire to assist reduction (as shown in the figure below).
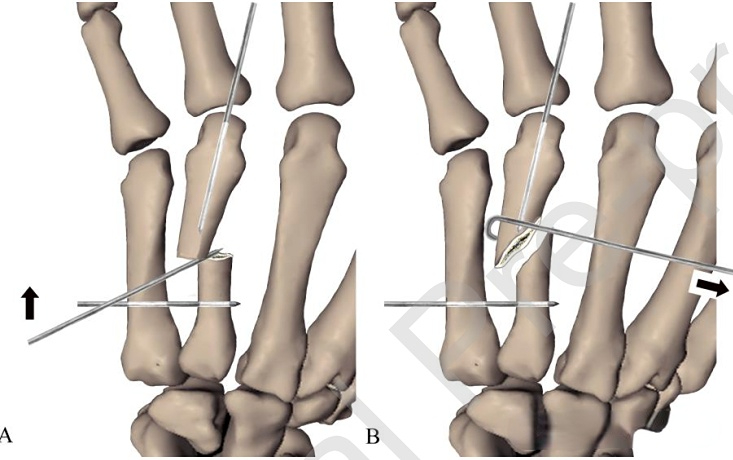
Step 3: After reduction, insert the distal intramedullary Kirschner wire directly into the medullary cavity of the proximal bone block to temporarily maintain reduction. After the position is satisfactory, insert two Kirschner wires through the fifth metacarpal bone to the distal bone block, and then insert one to fix the proximal end. After fixing two at the distal and proximal ends, remove the intramedullary fixation Kirschner wire. After fixation, the Kirschner wire is left outside the skin and the patient can return to work.
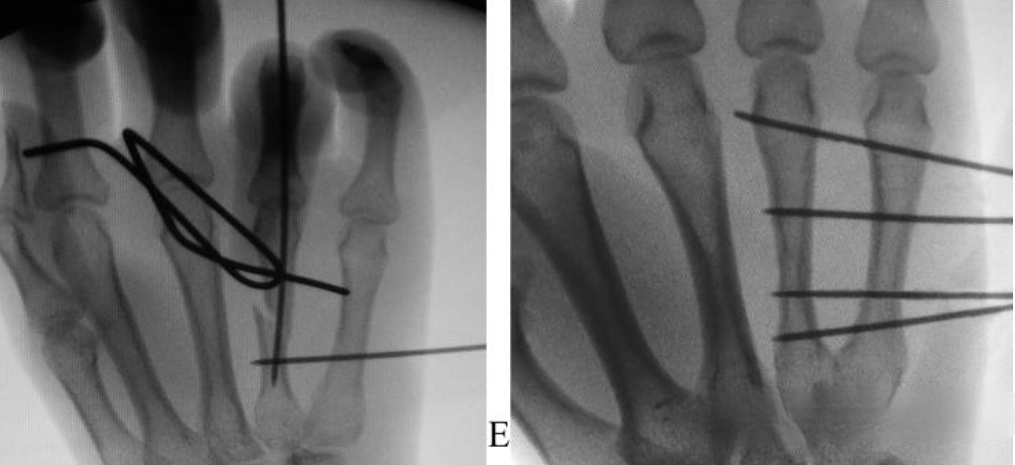
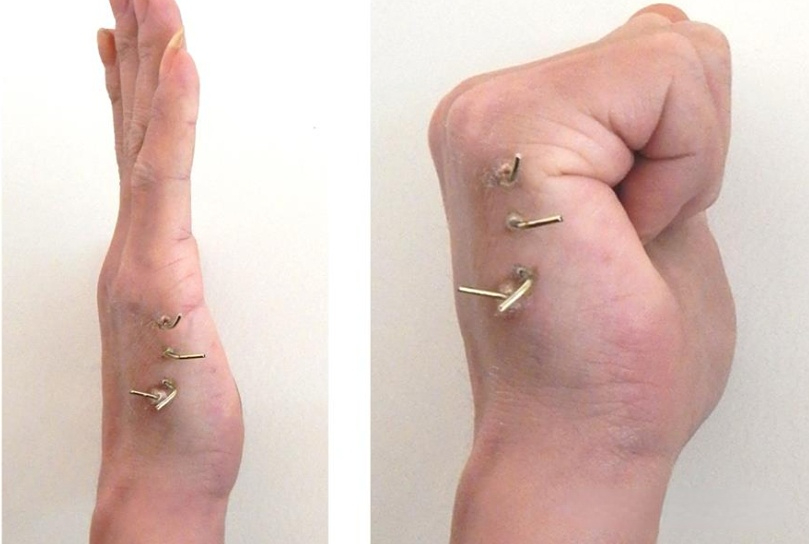
Plate screw fixation and Kirschner wire fixation for metacarpal fractures each have their own indications. Both the AO series of books and Green’s Hand Surgery describe in detail the plate screw internal fixation technique for metacarpal fractures. Even though the Kirschner wire surgery is minimally invasive, the fixation strength cannot be compared with the plate screw system, and the needle tail left outside the skin is still a psychological burden for the patient, and returning to work is still unavoidable. The problem of nail tract infection cannot be ruled out; the metacarpal plate system fixation can be performed under local anesthesia. Although there is a wound, it is not large. After bandaging, returning to work directly is not more difficult than Kirschner wire fixation. Therefore, doctors who like Kirschner wire fixation can choose Kirschner wire fixation; those who are good at plate screw fixation can also use this fixation method. It doesn’t matter whether it is right or wrong, and there is no need to praise one and criticize the other. Don’t go to extremes. For reference by clinical doctors.
[Statement]: The concepts, technologies, and principles shared on this platform are all publicly available journals, published books, or online platform materials. The copyright belongs to the original author. The platform only organizes, summarizes, and shares them for learning reference. This platform is not responsible for the authenticity of the content and the effectiveness of the technology. The related medical behaviors generated based on the content pushed by this platform have nothing to do with the platform. Please choose carefully. If there is any infringement, please contact us to delete it.
Welcome to share, forward and like the article in the lower right corner!