Distal humeral fractures account for 2% of all fractures in the body and 33% of humeral fractures, which are very challenging for surgeons. The elbow joint is one of the most complex joints, including the humero-ulnar joint, humeroradial joint, and superior radioulnar joint. The most common complications of distal humeral fractures are stiffness, nonunion, infection, ulnar nerve, and internal fixation. Distal humeral fractures are more common in young men and elderly women. The purpose of surgical treatment is to anatomically reduce the articular surface fracture and align it well with the epiphysis, and to achieve strong fixation so that active functional exercises can be performed as soon as possible after surgery.
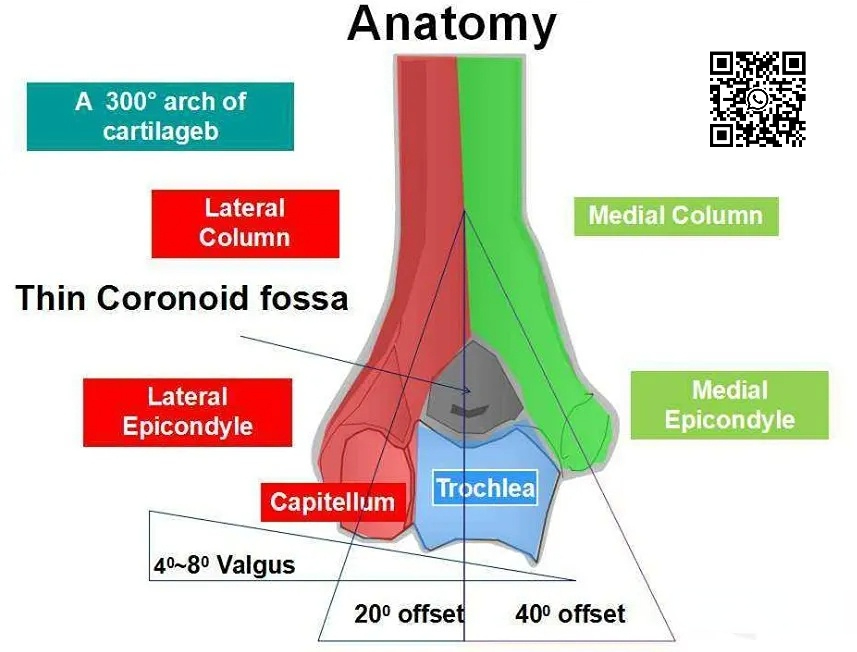
Anatomical features
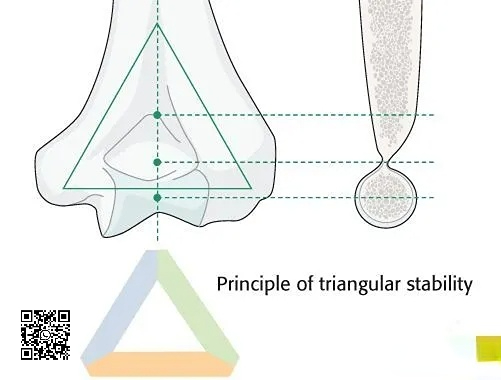
The two columns of the distal humerus and the central pulley form a stable bony triangle, with the olecranon fossa and coronoid fossa located in the center of the triangle. The anterior surface of the lateral column is the humeral head, and there is no articular surface behind it, where a plate is often placed. During surgical reduction, the restoration of the stable triangular structure must be completed.
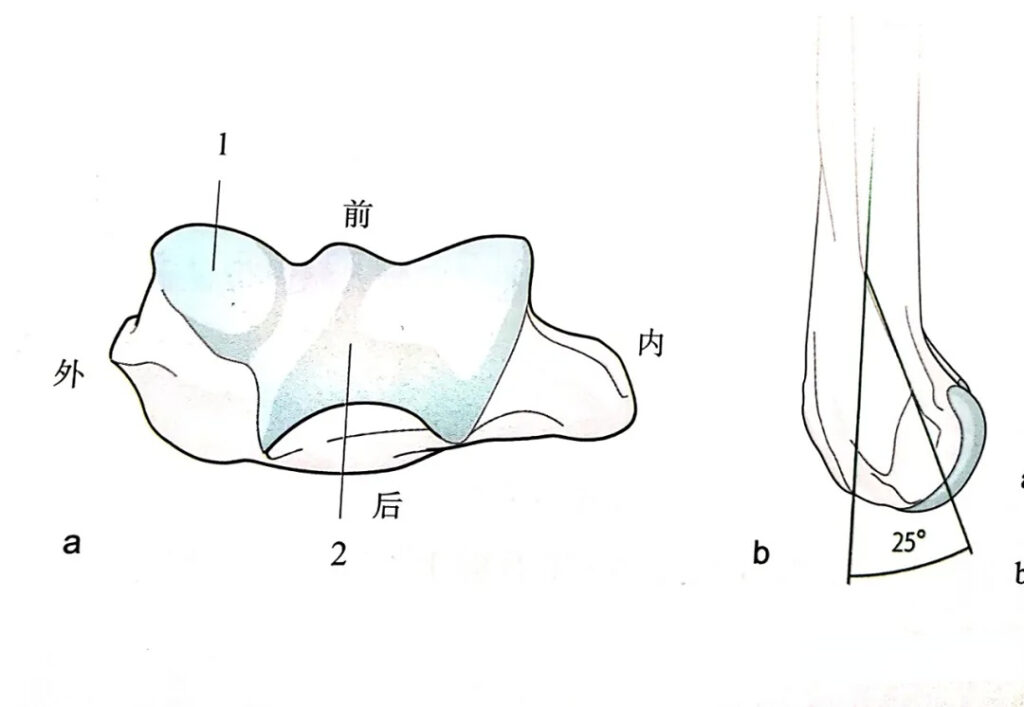
The axial pulley is located in the center rather than the medial side, and the rotation axis of the pulley is located in front of the humeral shaft and faces forward. The arc of the lateral column tilts forward to the level of the center of the rotation axis, while the medial column remains in the same straight line with the humeral shaft. Therefore, placing a straight plate on the posterolateral surface of the humerus will cause the distal humerus to lose its anteversion.
Injury mechanism
Direct violence: high-energy injury in young people; direct impact on the elbow joint of middle-aged and elderly people
Indirect violence: sports injury in young people; middle-aged and elderly people landing with their upper limbs straight
Fracture direction and force factors:
When flexion is less than 90°, the forearm receives the load, which is a single column or single condylar fracture;
When flexion is greater than 90°, the olecranon receives the load, which is a supracondylar or double-column comminuted fracture;
Classification
According to the AO classification, distal humeral fractures are divided into three types. Type A is an extra-articular fracture, Type B is a partially intra-articular fracture, and Type C is a completely intra-articular fracture. And according to the degree of fracture displacement, it is also divided into four types. Type 1 has no obvious displacement of the fracture end or a slight displacement of no more than 2mm, Type 2 has a displacement of more than 2mm to the outside of the fracture end, and Type 3 has a complete displacement of the fracture, resulting in an inward displacement of the articular surface. Type 4 is a case where the fracture is combined with elbow dislocation.
The classification mainly distinguishes between distal humeral fractures involving a single column or double column (from the bottom to the top of the olecranon/coronoid fossa), or fractures involving the articular surface and perhaps the medial epicondyle but not involving the column (humeral capitellum and trochlea fractures).
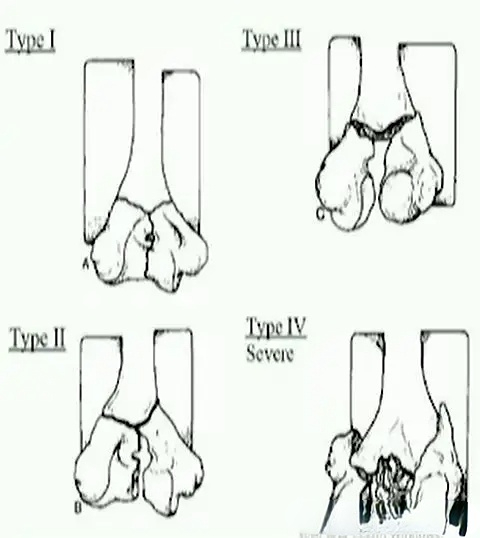
Riseborough classification
According to the degree of displacement, rotation and comminution of the fracture, it is divided into four categories:
Type I: fracture without separation and displacement
Type II: fracture with mild separation
Type III: both internal and external condyles have rotation and displacement
Type IV: articular surface has severe damage
This classification reflects the severity of the fracture and has guiding significance for judging the difficulty of surgery and prognosis, but it is insufficient in guiding specific treatment.
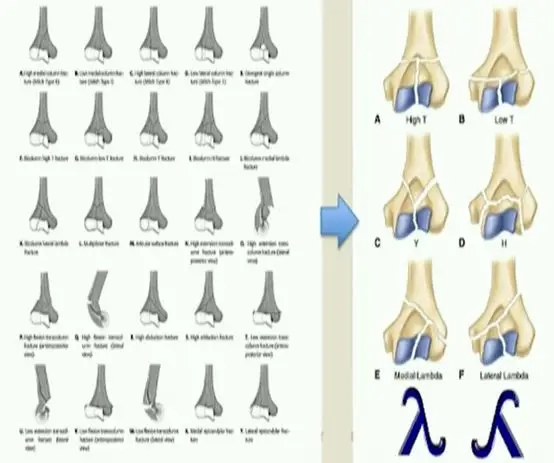
Jupiter-Mehne classification
Based on the anatomical concepts of double columns and arch bridges
Classification based on the range and morphology of the fracture line
Intra-articular fractures: single-column fractures, double-column fractures, fractures of the articular surface (capitellum and trochlea)
Extra-articular, intracapsular fractures
Fractures outside the joint capsule
Indications for surgery
Displaced intra-articular fractures.
Open fractures
Fractures with nerve damage
Multiple injuries
Distal Humerus Compression Locking Plate
Features
●No or only a small amount of bending is required
●Smooth and blunt surface to reduce soft tissue irritation
●Stable fixation can be achieved using the double plate 90° plate placement technique
●Angled stability screw system, 2.7/3.5mm locking screws, optimal force transmission
●2.7mm locking screws, up to 60mm long, for optimal fixation of distal fracture fragments
●Five distal fixation options can fix extremely distal fractures, especially for patients with osteoporosis
●Three screws to fix the capitellum
Indications
●Intra-articular distal humeral fractures, especially for patients with osteoporosis
●Distal humeral supracondylar fractures
●Distal humeral nonunion
Disclaimer:
This article and all articles on this website are for reference only by medical professionals; specific medical problems should be treated promptly. To ensure “originality” and improve delivery efficiency, some articles on this website are AI-generated and machine-translated, which may be inappropriate or even wrong. Please refer to the original English text or leave a message if necessary. Copyright belongs to the original author. If your rights are violated, please contact the backstage to delete them. If you have any questions, please leave a message through the backstage, or leave a message below this article. Thank you!
Like and share, your hands will be left with the fragrance!