Vascular injury in orthopaedic trauma

- Vascular injury in orthopedic trauma is challenging. The risk to life and limb can be high. Clinical signs initially can be subtle
- The incidence of vascular injury in orthopedic trauma was 1.6% for adults and 0.6% for pediatric patients (National Trauma Data Bank Analysis).
- Patients with extremity vascular injuries tend to be younger (average age, 30 years) and predominantly (70%-90%) male, even though this trend tends to change for elderly patients. Vascular injuries from blunt orthopedic trauma, such as fractures, dislocations, contusions, crush injuries, and traction, account for 5% to 25% of injuries that require treatment.
- The femoral or popliteal arteries are most commonly injured (50% to 60%), followed by the brachial artery (30%).
- The anatomy of the lower extremity predisposes the femoral and popliteal vessels to injury at certain locations during trauma. The popliteal artery runs through the popliteal fossa and is tethered proximally by the adductor hiatus and distally by the soleus arch. Therefore, high rates of vascular injuries are observed with specific lower-extremity injuries such as high-energy tibial plateau fractures, high-energy displaced distal femoral fractures at the level of the adductor hiatus, open fractures of the femur, segmental femoral fractures, floating knee injuries, and posterior knee dislocations
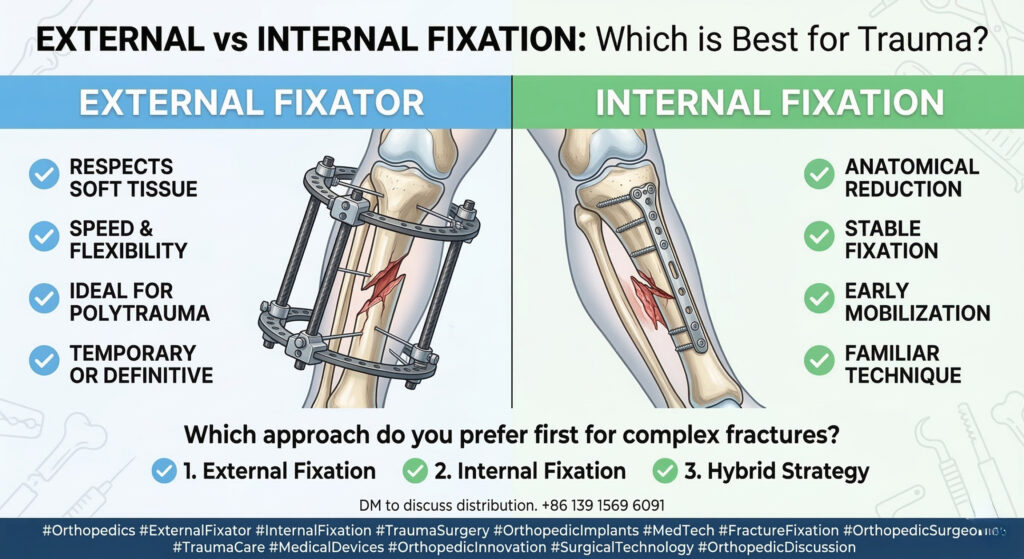
- In general, achieving bony stabilization greatly facilitates vascular reconstruction.
- Ischemia due to vascular injury is a major risk factor for amputation, and, ideally, the injury will be identified and treated within six hours to minimize ischemic nerve and muscle damage.
- External fixation is usually performed quickly; however, if any problems are foreseen, a vascular shunt can be placed before external fixation to limit warm ischemia time to the distal limb.
- Surgical management:
- Vascular ligation: ligation (arterial or venous) is best tolerated with distal or minor vascular injury. There is some degree of redundancy of circulation in the forearm and leg.
- Vascular shunting: typically used for larger, more proximal arteries and veins such as the femoral, popliteal, and brachial vessels. Prolonged disruption of flow proximally is associated with increased morbidity due to a greater burden of tissue ischemia compared with injury to more distal vessels. Vascular shunting may also be more crucial for injuries in which collateral circulation has been disrupted.
- A thorough vascular assessment is essential; an arterial pressure index <0.90 is indicative of potential vascular compromise. Advances in CT and duplex ultrasonography are sensitive and specific in screening for vascular injury. A patient with diminished peripheral pulses or an ABI less than 0.9 should undergo an imaging study, typically arteriography, Duplex US, or CT angiography (CTA) to document the presence and location of a possible vascular injury.
- Open vascular repairs, such as direct repair with or without arteriography, interposition replacement, and bypass graft with an autologous vein or polytetrafluoroethylene, remain the standard of care in managing vascular injury associated with extremity trauma. Although surgical technique affects outcome, results are primarily dependent on early detection of vascular injury followed by immediate treatment.
- Teamwork, familiarity with the often subtle signs of vascular injuries, a high index of suspicion, effective communication, appropriate use of imaging modalities, sound knowledge of relevant techniques, and sequence of surgical repairs are among the essential factors that will lead to a successful outcome.
References:
- Vascular Injury in Orthopedic Trauma. Mavrogenis AF. Orthopedics. 2016 Jul 1;39(4):249-59
- Vascular injury associated with extremity trauma: initial diagnosis and management. Halvorson JJ.
Disclaimer:
This article and all articles on this website are for reference only by medical professionals; specific medical problems should be treated promptly. To ensure “originality” and improve delivery efficiency, some articles on this website are AI-generated and machine-translated, which may be inappropriate or even wrong. Please refer to the original English text or leave a message if necessary. Copyright belongs to the original author. If your rights are violated, please contact the backstage to delete them. If you have any questions, please leave a message through the backstage, or leave a message below this article. Thank you!
Like and share, your hands will be left with the fragrance!