Proximal humeral fractures are very common in orthopedic clinical practice. This article will discuss several major pitfalls that need to be noted in open reduction and internal fixation and intramedullary nailing of proximal humeral fractures, aiming to provide guidance for young orthopedic surgeons to optimize surgical outcomes and reduce postoperative complications.
Open reduction and internal fixation of proximal humeral fractures
Missed GT and LT Fractures: GT fractures are often posteriorly displaced and may appear minimally displaced on AP radiographs. Impacted LT fractures commonly occur with posterior dislocations. Obtain axillary and transscapular radiographs and consider CT scans to accurately assess these fractures.
Ignoring Physiologic Age: Consider the patient’s physiologic age (activity level and demands) when making surgical decisions. A healthy, highly active elderly patient may benefit more from surgery than a younger, unhealthy, inactive patient.
Axillary Nerve Injury: The axillary nerve is at risk during both deltopectoral and deltoid split approaches. Identify and protect the nerve during dissection, retractor placement, and plate application to avoid injury.
Subacromial Impingement: When fixing GT fractures with screws, keep implants low on the tuberosity to avoid subacromial impingement with shoulder motion.
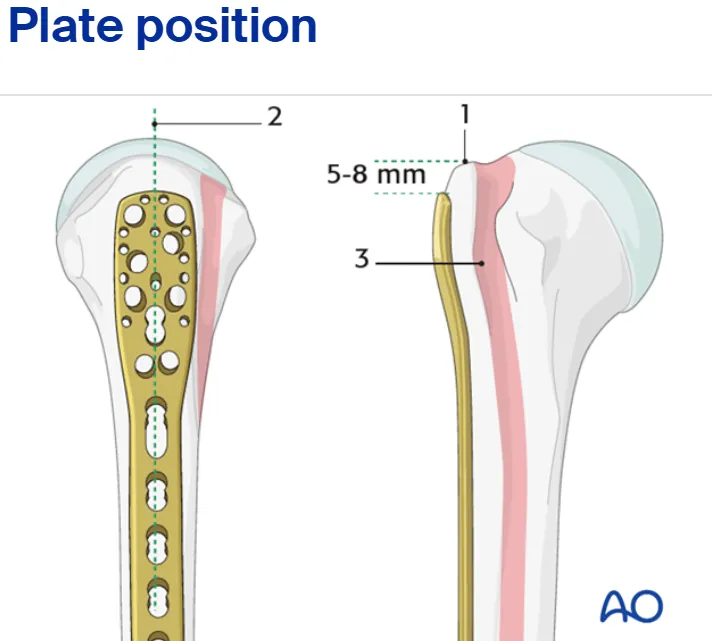
High Plate Placement: The most common error with plate fixation is placing it too high on the proximal humerus. This can cause subacromial impingement. Ensure the plate is positioned low to avoid this complication.
Drilling Through the Articular Surface: Do not drill through the articular surface of the humeral head. This increases the risk of screw penetration into the joint and can lead to varus collapse and arthritis.
Inadequate Tuberosity Fixation: Poor fixation of the tuberosities can lead to malunion, nonunion, and loss of shoulder function. Use a combination of screws, sutures, and/or tension band constructs to achieve secure fixation, paying attention to the quality of bone.
Intramedullary nailing of proximal humeral fractures
Medullary Canal Breach: Breaching the medullary canal can lead to neurovascular injury or misplacement/migration of the nail. Use gentle technique and follow the natural curvature of the humerus with awls and reamers.
Inadequate Medial Nail Insertion: Ensure the nail is inserted sufficiently into the medial fragment (at least 5 cm past the fracture) to provide adequate stability. Failure to do so can compromise fixation and lead to nonunion.
Prominent Nail Proximally: Avoid a prominent nail proximally, as this can cause rotator cuff irritation and subacromial impingement. Ensure the nail is appropriately countersunk.
Misaligned/Errant Reaming: Reaming should be performed with the fracture anatomically reduced and aligned. Any varus or translational malalignment during reaming will result in a similar deformity when the nail is inserted.
Distal Cortex Penetration: Avoid penetrating the distal humeral cortex with the nail, especially in osteoporotic bone. This can cause iatrogenic distal humeral fracture or pain. Choose the shorter of two nail lengths if unsure.
Screw Penetration: Avoid penetrating the subchondral bone of the humeral head with locking screws. This can lead to head collapse and screw protrusion into the joint.
Inadequate Proximal Screw Fixation: Use maximal (three to four) screw fixation rather than minimal screw fixation in the proximal humerus to provide better stability, particularly in osteoporotic bone.
Disclaimer:
This article and all articles on this website are for reference only by medical professionals; specific medical problems should be treated promptly. To ensure “originality” and improve delivery efficiency, some articles on this website are AI-generated and machine-translated, which may be inappropriate or even wrong. Please refer to the original English text or leave a message if necessary. Copyright belongs to the original author. If your rights are violated, please contact the backstage to delete them. If you have any questions, please leave a message through the backstage, or leave a message below this article. Thank you!
Like and share, your hands will be left with the fragrance!