Segmental tibial fractures are complex injuries involving two or more distinct fracture lines and a free-floating middle fragment. This complexity demands a multidisciplinary approach and careful consideration of various factors when deciding on the optimal treatment. Here’s a breakdown of common treatment methods and their pros and cons:
1. Non-operative Treatment:
- Method: Cast immobilization or skeletal traction.
- Advantages: Minimal invasive, avoids surgery-related complications.
- Disadvantages:
- Ineffective: Often fails to achieve and maintain adequate alignment.
- High Risk: Increased risk of malunion, nonunion, and shortening due to fracture instability.
- Prolonged Immobilization: This can lead to joint stiffness and muscle atrophy.
- Suitable for: Rarely indicated due to poor outcomes. May be considered for minimally displaced, stable fractures in patients with significant medical comorbidities.
2. Surgical Treatment:

a) Intramedullary Nailing (IMN):
- Method: Reamed or undreamed nail inserted into the medullary canal. Locking screws secure the nail proximally and distally.
- Advantages:
- Biomechanically Stable: Provides excellent stability for early weight-bearing and mobilization.
- Minimally Invasive: Reduced soft tissue dissection compared to plating.
- Disadvantages:
- Deep Infection Risk: Increased risk, especially in open fractures, potentially leading to nonunion and amputation.
- Rotational Malalignment: The intermediate segment can spin during reaming, potentially causing soft tissue damage and nonunion.
- Requires Expertise: Demands technical proficiency for accurate nail placement and locking screw insertion.
- Suitable for:
- Closed Fractures: Generally preferred for stable fixation and faster union.
- Open Fractures: Controversial due to infection risk, but reamed nailing may be favored in stable type I and II open fractures.
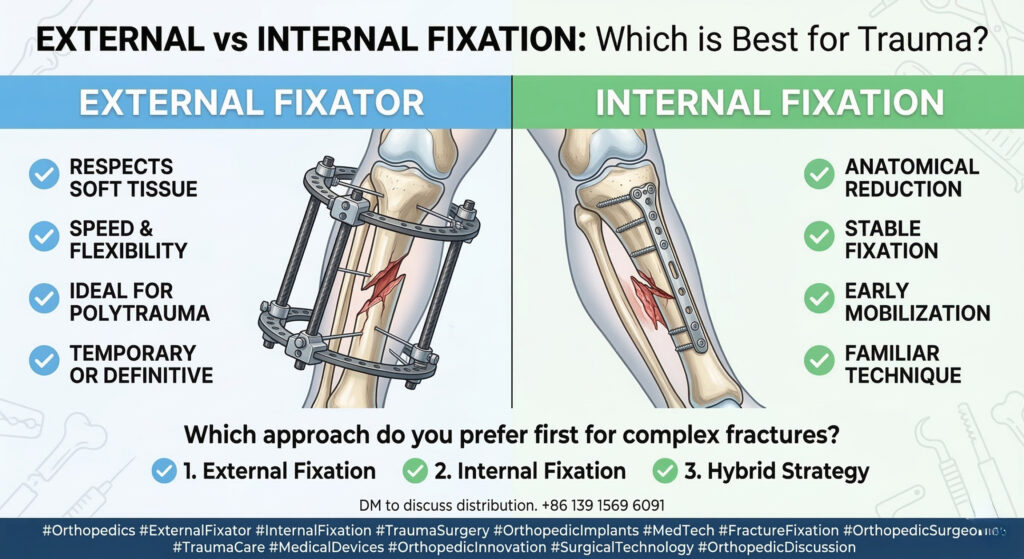
b) Open Reduction and Internal Fixation (ORIF) with Plating:

- Method: Direct exposure of fracture fragments and fixation with plates and screws.
- Advantages:
- Direct Visualization: Allows accurate anatomical reduction and fixation.
- Versatile: Can address complex fracture patterns and bone defects.
- Disadvantages:
- Extensive Soft Tissue Dissection:
Increased risk of infection, devascularization, and wound healing problems. - Implant Prominence: Plates can be prominent, causing discomfort and requiring removal.
- Delayed Weight-Bearing: May delay mobilization and functional recovery.
- Extensive Soft Tissue Dissection:
- Suitable for:
- Complex Fractures: May be preferred for fractures with comminution, bone loss, or intra-articular involvement.
- Open Fractures: Not generally preferred unless necessary for achieving stable fixation.
c) Circular External Fixation (CEF):
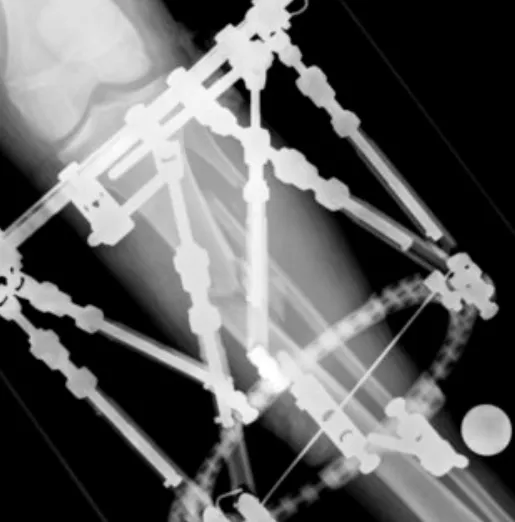
- Method: Circular frame with wires or half-pins inserted percutaneously into bone segments. Adjustable struts allow for gradual correction of deformity.
- Advantages:
- Minimally Invasive: Preserves soft tissue envelope and blood supply, reducing infection risk.
- Adjustable: 可调节: Allows for gradual correction of deformity and limb lengthening.
- Versatile: 多功能: Can manage open fractures with significant soft tissue damage and bone loss.
- Disadvantages:
- Pin-Site Infections: Common complication requiring meticulous pin care.
- Patient Discomfort: A bulky frame can be cumbersome and uncomfortable.
- Prolonged Treatment: May require a longer time to achieve union.
- Suitable for:
- Open Fractures: Preferred for severe open fractures with significant soft tissue damage (Gustilo-Anderson type IIIB and IIIC).
- Complex Fractures: Effective for managing bone defects and malunion.
Choosing the Optimal Treatment
The choice of treatment depends on several factors:
- Fracture Type: Closed vs. open, fracture pattern, degree of comminution, bone loss, and articular involvement.
- Soft Tissue Injury: Severity of soft tissue damage, wound contamination, and vascularity.
- Patient Factors: Age, medical comorbidities, smoking status, and compliance.
- Surgeon Expertise: Familiarity and experience with different fixation techniques.
Summary and Recommendations:
- Reamed IMN: Generally preferred for closed segmental tibial fractures due to its stability and faster union rates.
- CEF: Recommended for severe open fractures and those with significant soft tissue damage.
- ORIF: Reserved for complex fracture patterns or situations where IMN and CEF are not feasible.
Open communication and shared decision-making between the surgeon and patient are crucial for choosing the most appropriate treatment, considering individual circumstances and priorities.
Disclaimer:
This article and all articles on this website are for reference only by medical professionals; specific medical problems should be treated promptly. To ensure “originality” and improve delivery efficiency, some articles on this website are AI-generated and machine-translated, which may be inappropriate or even wrong. Please refer to the original English text or leave a message if necessary. Copyright belongs to the original author. If your rights are violated, please contact the backstage to delete them. If you have any questions, please leave a message through the backstage, or leave a message below this article. Thank you!
Like and share, your hands will be left with the fragrance!