Why Medial Malleolus Fixation Matters More Than Most Surgeons Think
Ankle fractures are among the most common injuries encountered in orthopedic trauma surgery. Yet many fixation failures do not occur because surgeons fail to reduce the fracture. They occur because the wrong implant is selected for the wrong fracture pattern.
The ankle is unforgiving.
Unlike many joints, even minimal incongruity can significantly alter contact pressures within the tibiotalar articulation. A few millimeters of displacement may accelerate cartilage degeneration and ultimately contribute to post-traumatic osteoarthritis.
This reality becomes even more important as populations age and osteoporosis becomes increasingly prevalent. Surgeons are now treating more complex fracture patterns in patients with poorer bone quality than ever before.
Choosing the correct medial malleolus fixation strategy is not merely a technical decision. It is a biological and biomechanical decision that may influence ankle function for decades.
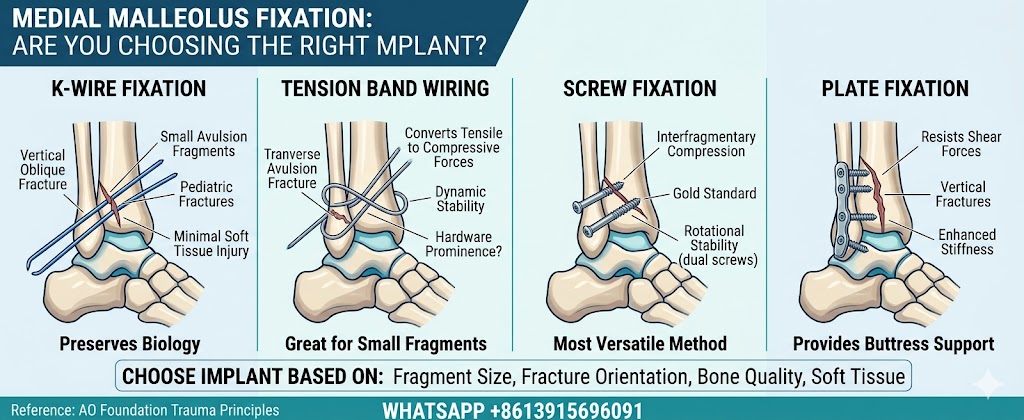
According to guidance from the AO Foundation, fixation methods should be selected based on fragment size, fracture orientation, bone quality, and soft tissue conditions—not surgeon preference alone.
K-Wire Fixation Still Has a Place in Modern Ankle Surgery
Many surgeons dismiss Kirschner wires as outdated technology.
That view is shortsighted.
While K-wire fixation cannot compete with modern plate constructs in terms of rigidity, there remain situations where it offers distinct advantages. Small avulsion fragments, pediatric fractures, and cases involving open physes often benefit from this simple approach.
In rotational ankle injuries, the strong deltoid ligament can generate avulsion-type fractures at the medial malleolus. Some fragments are simply too small to accommodate conventional hardware.
For skeletally immature patients, preserving the growth plate becomes critical. K-wires allow stabilization while minimizing physeal injury risk.
Biomechanical investigations have shown improved construct stability when:
- Three wires are utilized
- Two cross into the opposite cortex
- One remains parallel to the physis
This configuration enhances resistance to displacement while preserving biological integrity.
Sometimes the simplest solution remains surprisingly effective.
Tension Band Wiring—Old Technique, New Relevance
Few fixation methods generate as much debate as tension band wiring.
Supporters point to its ability to stabilize tiny fragments that cannot reliably accommodate screws. Critics highlight frequent hardware irritation and secondary implant removal procedures.
Both sides are correct.
AO principles continue to recommend tension band constructs for small avulsion fractures because they convert tensile forces into compression during ankle motion. This mechanism creates dynamic stability that can outperform expectations.
Several clinical studies have reported excellent union rates and strong fixation strength when compared with conventional lag screw techniques.
However, there is a cost.
Patients frequently report:
- Prominent hardware
- Soft tissue irritation
- Pain during footwear use
- Secondary surgery requirements
More recent randomized studies suggest that headless compression screws may achieve similar healing outcomes while reducing symptomatic implants.
The debate is far from over, but tension band constructs remain highly relevant when fragment size limits alternative options.
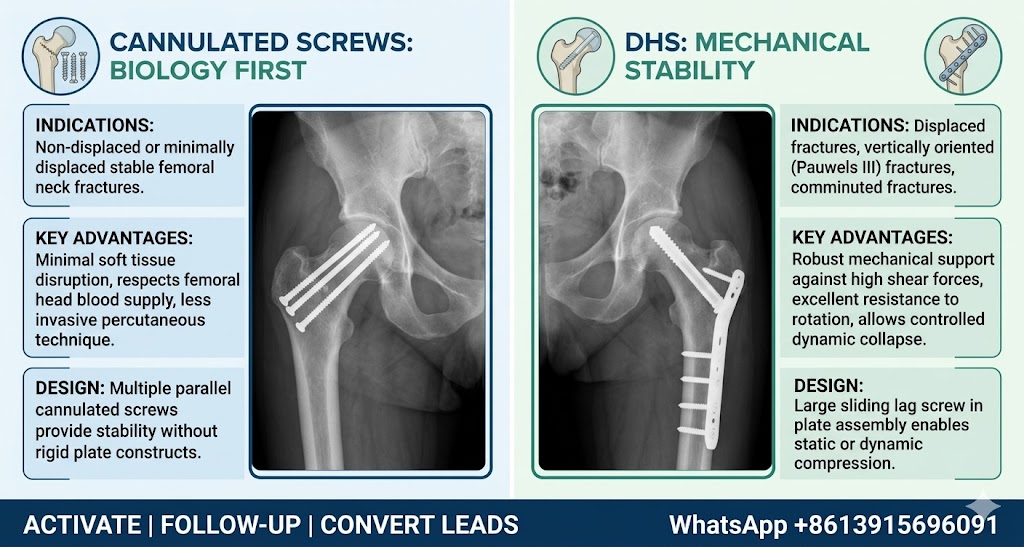
Why Screw Fixation Remains the Gold Standard
For most fracture configurations, screw fixation remains the benchmark against which all other methods are measured.
The reason is straightforward.
Compression promotes healing.
Properly placed lag screws generate interfragmentary compression, maintain reduction, and preserve soft tissue integrity. This combination explains why screw fixation continues to dominate ankle trauma surgery.
Today’s options include:
- Headless compression implants
- Partially threaded cancellous screws
- Fully threaded bicortical devices
Recent biomechanical studies have challenged traditional thinking. Evidence suggests that fully threaded bicortical constructs may provide superior resistance to displacement compared with conventional partially threaded designs.
Another controversial topic involves single versus dual screw fixation.
While clinical outcomes often appear similar, biomechanics tell a different story. A single implant controls compression but offers less rotational resistance. Two fixation points create a more stable environment and may reduce fragment rotation during rehabilitation.
In fracture management, controlling torsion is often as important as generating compression.
Vertical Shear Fractures Demand a Different Strategy
Not every injury behaves according to textbook rules.
Vertical shear fractures represent one of the most demanding patterns encountered around the ankle.
These injuries generate substantial translational forces. Traditional lag screw constructs may struggle to resist displacement, particularly under cyclical loading conditions.
This is where plate fixation becomes valuable.
A buttress construct functions differently from compression-based fixation. Instead of simply pulling fragments together, it physically blocks shear movement.
Several studies have demonstrated that plate constructs offer superior mechanical stability in vertical fracture patterns compared with isolated screws.
Advantages include:
- Enhanced resistance to shear forces
- Improved fragment control
- Greater construct stiffness
- Better support in osteoporotic bone
The disadvantages are equally important.
Plate fixation often requires:
- Larger exposure
- Greater periosteal stripping
- Increased hardware prominence
- Potential wound complications
Therefore, plating should not be routine. It should be reserved for fracture patterns where biomechanics clearly justify the additional soft tissue compromise.
Matching the Implant to the Fracture Is the Real Secret
There is no universal implant.
There never will be.
The future of medial malleolus fracture treatment lies in personalization rather than standardization.
A practical decision framework may look like this:
Small Avulsion Fragment
- Tension band construct
- Kirschner wire stabilization
Pediatric Injury
- Physeal-sparing wire fixation
Standard Oblique Fracture
- Compression-based screw construct
Vertical Shear Pattern
- Buttress plate support
Osteoporotic Bone
- Enhanced fixation strategy with greater mechanical resistance
The most successful surgeons do not ask:
“What implant do I always use?”
They ask:
“What implant does this fracture require?”
That difference separates routine fixation from truly intelligent trauma surgery.
The implant itself rarely determines success.
The decision behind it does.
Reference
AO Foundation Trauma Principles:
https://www.aofoundation.org