Why Cannulated Screws vs DHS Is a High-Stakes Decision
Young femoral neck fracture is not a small injury. It is a surgical trap. One wrong fixation choice can turn a healthy hip into nonunion, femoral neck shortening, avascular necrosis, or early arthroplasty. That is why the debate around cannulated screws vs DHS in young femoral neck fractures remains so intense.
The real problem is not the implant name. It is the fracture biology. The femoral head depends heavily on the medial femoral circumflex artery, and displacement can damage that blood supply before the surgeon even starts. At the same time, vertical fracture patterns create powerful shear forces that small screws may not control.
So the question is sharp: should you protect blood supply with a less invasive construct, or fight instability with stronger mechanics?
Why Cannulated Screws Remain Popular in Young Femoral Neck Fractures
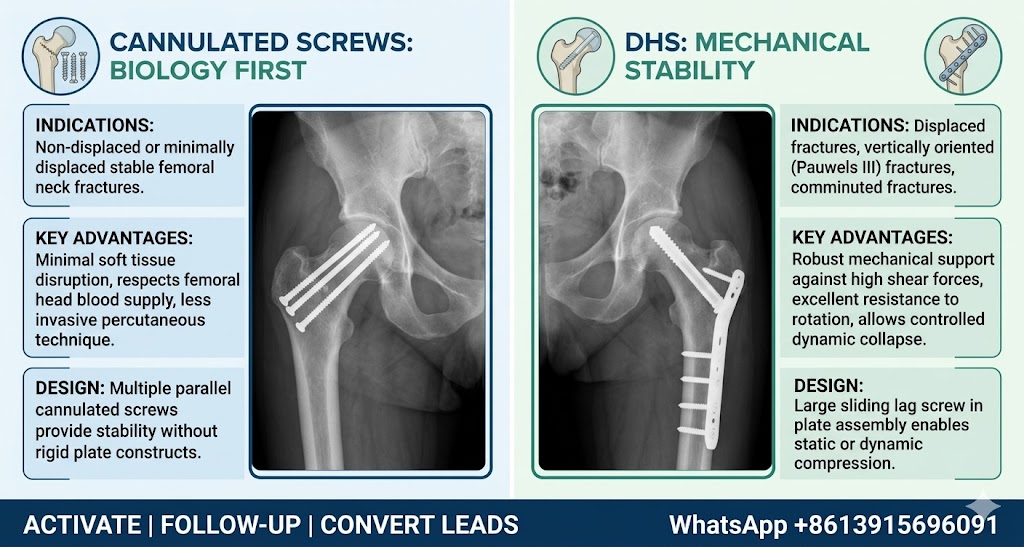
Cannulated screw fixation remains widely used because it respects biology. The technique is usually percutaneous, soft tissue disruption is limited, and the operation can be efficient when reduction is clean. For young patients, that matters. Their goal is not merely union; they need a preserved femoral head and a functional hip for decades.
The classic inverted triangle configuration provides controlled support within the femoral neck. In stable patterns, this can be enough. The best indications include:
- Garden I–II fractures
- Pauwels I–II fractures
- Good bone quality
- Minimal displacement
- Low shear force across the fracture line
Here, cannulated screws offer a strong balance: limited surgical trauma, flexible screw positioning, and lower interference with remaining vascular structures. But this advantage has a ceiling. When the fracture becomes vertical, displaced, or rotationally unstable, biology-friendly fixation may become mechanically weak.
When DHS Becomes the Stronger Mechanical Option
Dynamic Hip Screw (DHS) fixation enters the debate when fracture stability becomes the dominant threat. In Pauwels III femoral neck fractures, the fracture line is more vertical, and the load across the fracture turns from compression into shear. That changes everything.
Multiple small screws may slide, loosen, or allow femoral neck shortening. DHS uses a larger sliding hip screw connected to a lateral plate, creating a more powerful construct against shear. It also permits dynamic compression during controlled loading, which may help fracture healing when the reduction is accurate.
DHS is often favored in:
- Vertical shear fractures
- Displaced femoral neck injuries
- High-energy trauma cases
- Young patients with unstable fracture geometry
- Cases requiring an additional anti-rotation screw
The trade-off is real. DHS usually requires a larger incision, more soft tissue handling, and potentially greater disturbance around the hip. That is why using DHS in every case would be blunt and excessive. In stable fractures, it may be too much metal for too little need.
The Real Decision: Fracture Stability Comes First
The mistake is asking, “Which implant is better?”
That question is too shallow.
The sharper question is: what mechanical problem does this fracture create?
If the fracture is stable, non-displaced, and low shear, cannulated screws usually make sense. They preserve soft tissue, reduce operative trauma, and provide adequate fixation. If the fracture is vertical, displaced, or clearly unstable, DHS becomes more persuasive because mechanical failure is the greater danger.
A practical decision map looks like this:
- Garden I–II: cannulated screws are usually preferred
- Garden III: choose based on reduction quality and residual stability
- Pauwels III: DHS often provides better shear resistance
- Highly unstable pattern: DHS plus anti-rotation screw may be considered
The implant should follow the fracture. Not the surgeon’s habit.
What the Evidence Says About Cannulated Screws vs DHS
Evidence does not support blind loyalty to either method. Parker and Stockton reviewed internal fixation options for intracapsular proximal femoral fractures and found that multiple implants can work when indications are correct. Baitner and colleagues showed that vertical shear femoral neck fractures create a mechanical environment where DHS can outperform multiple screws in stability. Slobogean and co-authors later emphasized that complications in young femoral neck fractures remain significant, especially when fracture displacement and instability are present.
For further reading, see related literature through PubMed: https://pubmed.ncbi.nlm.nih.gov/
The evidence points toward a practical conclusion: in stable femoral neck fractures, cannulated screws remain a rational choice. In high-shear or unstable patterns, DHS may reduce fixation failure by offering superior mechanical control.
Case Logic: Two Fractures, Two Different Answers
Consider a 34-year-old patient with a Garden II femoral neck fracture after a traffic accident. The fracture is minimally displaced, the line is relatively horizontal, and reduction is satisfactory. In this case, three cannulated screws in a triangular configuration can provide stable fixation while preserving soft tissue and vascular structures. The goal is elegant: stabilize without over-treating.
Now consider a 39-year-old patient after a fall from height. Imaging shows a Pauwels III fracture, vertical orientation, and clear displacement. This is not the same injury. The shear force is aggressive. Here, DHS with an anti-rotation screw may offer a more reliable mechanical environment. Less invasive fixation may look attractive, but weak fixation in a high-shear fracture is a bad bargain.
Same anatomical region. Different mechanics. Different answer.
Common Mistakes Surgeons Must Avoid
Young femoral neck fracture management fails when surgeons underestimate instability. A beautiful small incision does not compensate for poor mechanics. Likewise, a strong implant does not rescue bad reduction.
Avoid these errors:
- Choosing cannulated screws for a clearly vertical shear fracture
- Ignoring femoral neck shortening risk
- Treating Garden classification without evaluating Pauwels angle
- Overusing DHS in stable, low-shear injuries
- Assuming fixation choice matters more than reduction quality
Reduction remains the foundation. Implant selection is the second decision, not the first. If the fracture is poorly reduced, both cannulated screws and DHS can fail.
Final Verdict: Biology Heals, Mechanics Protects
The debate over cannulated screws vs DHS in young femoral neck fractures should not be reduced to a brand-like preference. Cannulated screws are excellent for stable, low-shear fractures where biological preservation is the priority. DHS is stronger for vertical, displaced, or unstable injuries where shear resistance determines survival.
The best fixation is not the smallest implant. It is not the strongest implant either. It is the one that matches the fracture’s mechanical personality while protecting the femoral head’s biology.
In young patients, failure is expensive. The native hip is worth fighting for.