Bone traction techniques are essential skills in trauma orthopedics, particularly for managing complex fractures and joint dislocations. This article provides a detailed breakdown of the four major bone traction methods—supracondylar femoral traction, tibial tubercle traction, calcaneal traction, and olecranon traction—covering their indications and step-by-step procedures. Whether you are a seasoned orthopedic surgeon or a medical trainee, this guide will enhance your understanding and execution of these critical techniques.
1. Supracondylar Femoral Traction
Indications
Supracondylar femoral traction is commonly used for:
- Displaced femoral fractures.
- Displaced pelvic ring fractures.
- Central dislocation of the hip joint or chronic posterior hip dislocations.
- Preoperative preparation for chronic hip dislocation or congenital hip dislocation where soft tissue contractures cause deformity, especially when skin traction fails.
- Cases where prolonged tibial tubercle traction results in pin loosening or pinhole infection, necessitating pin replacement.
Step-by-Step Procedure
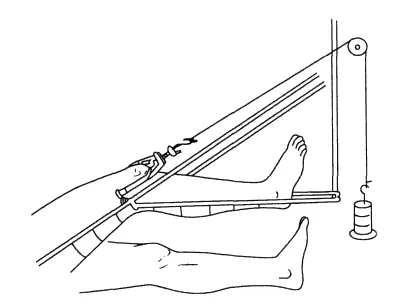
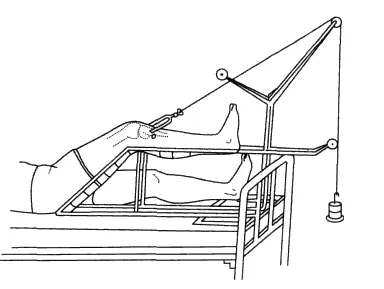
- Place the injured lower limb on a Brown traction frame.
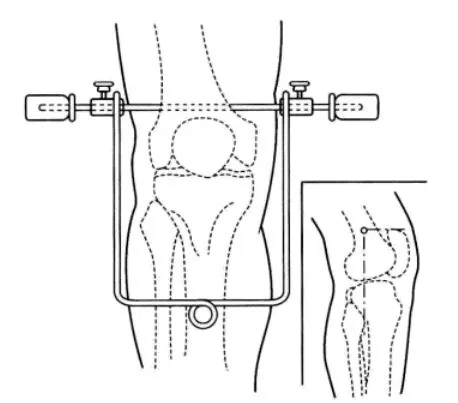
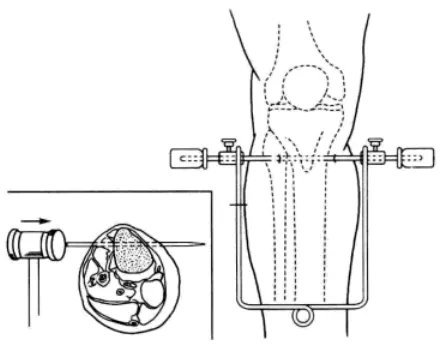
- Draw a horizontal line 1 cm proximal to the superior edge of the patella, perpendicular to the femur.
- Tip: For elderly patients with osteoporosis, place the pin slightly higher to avoid fractures. For younger patients with stronger bones, place it closer to the patella.
- Draw vertical lines along the fibular head and the highest point of the femoral medial condyle, intersecting the horizontal line. These intersections mark the entry and exit points for the Steinmann pin or Kirschner wire.
- After sterilization and local anesthesia, insert the pin from the medial entry point, ensuring it passes perpendicular to the femur and exits at the lateral mark.
- Caution: Protect the adductor hiatus to avoid damaging the femoral vessels and nerves.
- Ensure the pin is level and equidistant on both sides. Flatten the skin around the pin entry using towel clamps to prevent soft tissue depression.
- Attach the traction bow and commence traction on the frame.
- Elevate the foot of the bed by 20–25 cm to provide countertraction.
- Adjust the traction weight based on the patient’s weight and injury severity:
- For pelvic fractures, femoral fractures, or hip dislocations, use 1/7 to 1/8 of the patient’s body weight.
- For elderly or frail patients, reduce to 1/9 of body weight.
Key Points: Always insert the pin medial to lateral, perpendicular to the femur. Avoid anterior pin placement to prevent entry into the suprapatellar bursa or joint capsule.
2. Tibial Tubercle Traction
Indications
This technique is widely used for:
- Displaced femoral fractures.
- Pelvic ring fractures.
- Central hip dislocations and chronic hip dislocations.
Tibial tubercle traction is favored for its simplicity, safety, and reliability.
Step-by-Step Procedure
- Place the injured limb on a Brown traction frame, and have an assistant stabilize the ankle to minimize pain and prevent secondary injuries.
- Choose one of two pin insertion techniques:
- First Method:
- Draw a horizontal line 1 cm below the tibial tubercle, perpendicular to the tibial axis.
- Mark two vertical lines 3 cm on either side of the tibial axis, creating two intersection points for pin insertion.
- Adjust placement according to bone quality:
- For osteoporotic patients, move the entry point downward to avoid avulsion fractures.
- For younger patients, move the entry point upward to prevent splintering.
- Second Method:
- Use the midpoint of the line connecting the tibial tubercle and the fibular head as the lateral entry point, with the corresponding medial point as the exit.
- Sterilize, anesthetize, and insert the Steinmann pin or Kirschner wire from the lateral entry point to the medial exit.
- Caution: Insert laterally to medially to avoid injury to the common peroneal nerve.
- Attach the traction bow and commence traction.
- Regularly monitor limb length, distal sensation, motor function, and blood supply, particularly during the first two weeks.
Key Points: The traction weight and technique are similar to supracondylar femoral traction. Ensure precise pin placement to avoid complications.
3. Calcaneal Traction
Indications
Calcaneal traction is ideal for:
- Unstable tibial and fibular fractures when closed reduction fails.
- Fractures with severe soft tissue injuries or compartment syndrome.
- Certain calcaneal fractures.
- Early treatment of mild hip or knee contractures.
Step-by-Step Procedure
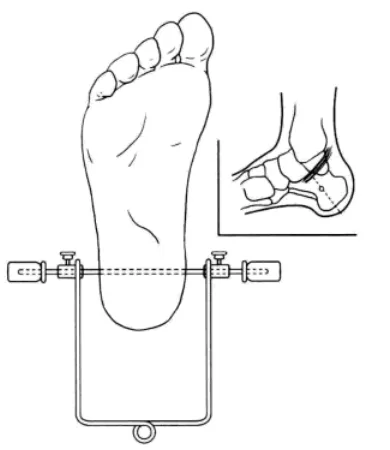
- Position the ankle in a neutral position.
- Identify the midpoint of the line connecting the medial malleolus and the posterior inferior edge of the heel as the entry point.
- After sterilization and local anesthesia, insert a Steinmann pin from the medial mark, ensuring it exits at the corresponding lateral mark.
- Caution: Avoid damaging the tarsal tunnel, posterior tibial artery, or tendons.
- Attach the traction bow and commence traction on the Brown frame.
- For fractures with severe displacement, apply a short leg cast for stabilization before traction.
- Use a traction weight of 4–6 kg for adults. Regularly check for toe movement, sensation, and circulation.
Key Points: Improper pin placement can cause complications:
- Pins placed too posteriorly may lead to equinus deformity.
- Pins placed too inferiorly risk exiting the bone.
- Pins placed too superiorly may enter the ankle joint capsule or damage tendons.
4. Olecranon Traction
Indications
Olecranon traction is primarily used for:
- Displaced humeral neck, shaft, or supracondylar fractures.
- Severe swelling that prevents immediate reduction.
- Chronic shoulder dislocations requiring closed reduction.
Step-by-Step Procedure
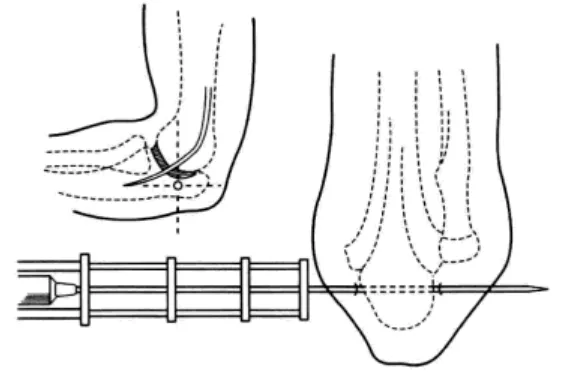
- Identify the entry point by drawing a line 3 cm distal to the olecranon tip, perpendicular to the ulnar dorsal edge.
- After sterilization and local anesthesia, insert a Kirschner wire from the medial mark, ensuring it exits at the corresponding lateral mark.
- Caution: Avoid damaging the ulnar nerve or entering the joint capsule.
- Attach the traction bow and secure the pin ends with adhesive tape to prevent loosening.
- Maintain the elbow at a 90° flexion angle using a sling. Apply a traction weight of 2–4 kg.
Key Points: Ensure proper pin alignment and monitor for nerve injuries or joint complications.
Conclusion: Mastering Bone Traction Techniques
Bone traction techniques like supracondylar femoral traction, tibial tubercle traction, calcaneal traction, and olecranon traction are indispensable in orthopedic trauma management. By adhering to precise indications and step-by-step protocols, surgeons can minimize complications and optimize patient outcomes.
For more detailed orthopedic guidelines, visit Orthobullets.
Meta Description:
Explore the four major bone traction techniques—supracondylar femoral, tibial tubercle, calcaneal, and olecranon traction. Learn their indications, step-by-step procedures, and expert tips for successful orthopedic management.
Disclaimer:
This article and all articles on this website are for reference only by medical professionals; specific medical problems should be treated promptly. To ensure “originality” and improve delivery efficiency, some articles on this website are AI-generated and machine-translated, which may be inappropriate or even wrong. Please refer to the original English text or leave a message if necessary. Copyright belongs to the original author. If your rights are violated, please contact the backstage to delete them. If you have any questions, please leave a message through the backstage, or leave a message below this article. Thank you!
Like and share, your hands will be left with the fragrance!