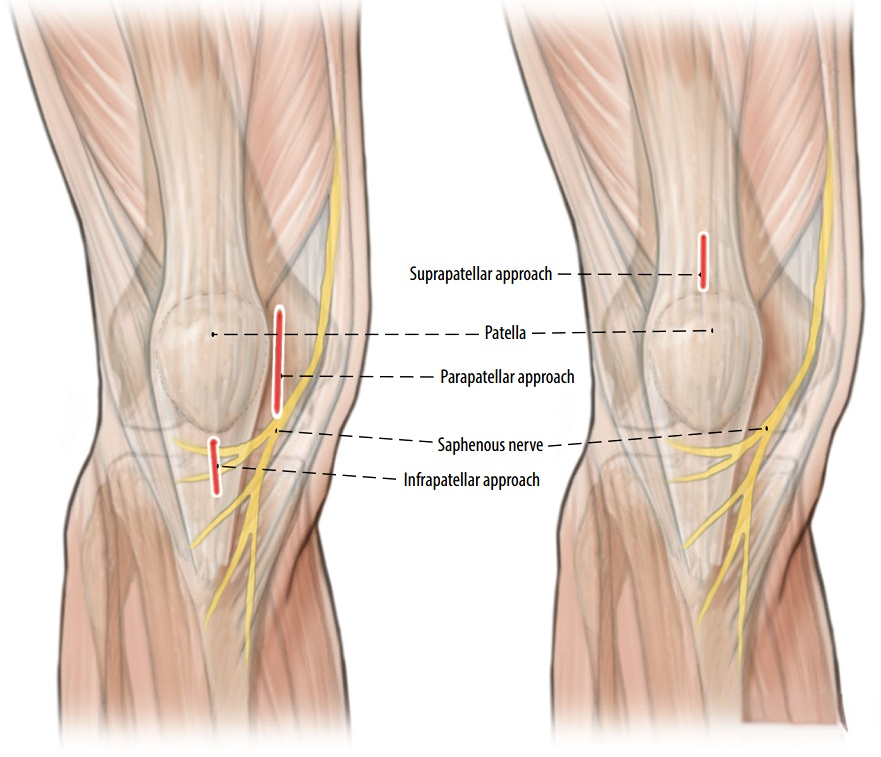
Intramedullary nailing of long bone #fractures has become the gold standard. For most #tibial shaft fractures, the infrapatellar approach is applicable to intramedullary nailing. However, for some special types, such as patients with infection of the proximal 1/3, the distal end, or the infrapatellar nailing point, or patients with limited knee flexion, it is difficult to fix them using the infrapatellar approach or the medial parapatellar approach. In this case, the suprapatellar approach can be used.
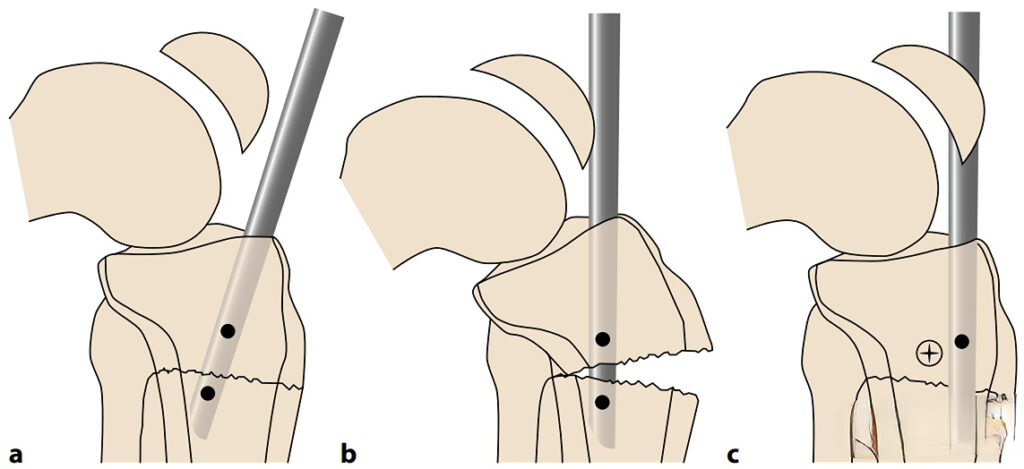
For proximal tibial fractures, the infrapatellar approach requires knee flexion, and the intramedullary nail collides with the posterior cortex, resulting in an opening in the front of the fracture, making it difficult to insert the main nail.
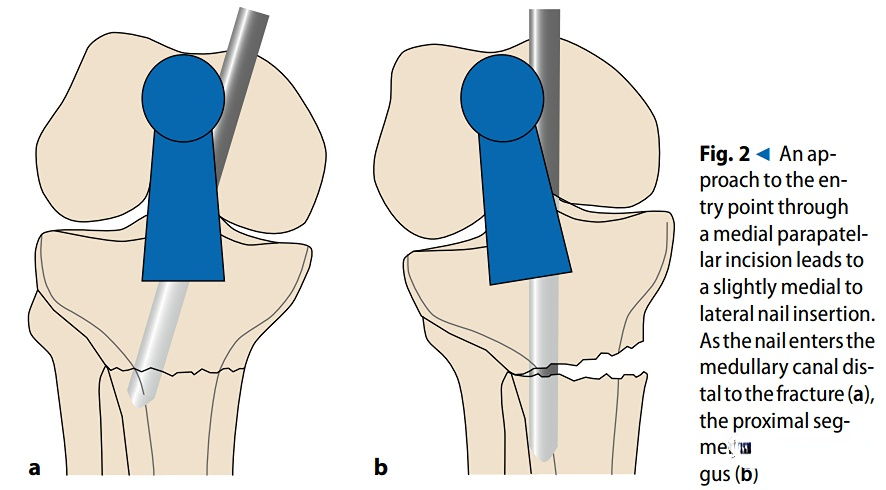
The insertion direction of the main nail through the medial #parapatellar approach is slightly outward, which may cause valgus deformity of the fracture end.
At the same time, the infrapatellar incision and the medial parapatellar incision have a higher risk of saphenous nerve injury compared with the suprapatellar incision.
Indications for the suprapatellar approach:
Extra-articular fracture of proximal tibia (AO 41A);
Simple or comminuted fracture of a the tibial shaft (AO 42A-C);
Multi-segmental fracture of a the tibial shaft (AO 42C);
Extra-articular fracture of distal tibia, or simple fracture of distal tibia extending to the articular surface (AO 43A C1);
Floating knee injury;
Calcification of patellar tendon;
Contamination of wound at the level of needlepoint
Contraindications:
Gustilo IIIC type open fracture;
Soft tissue injury, contamination, or soft tissue infection at suprapatellar needlepoint;
Presence of ipsilateral knee prosthesis (relative contraindication);
Presence of tibial plateau fracture at the needle point (relative contraindication);
Implant blocking the needlepoint;
Ipsilateral patellar fracture (relative contraindication)
Surgical procedures
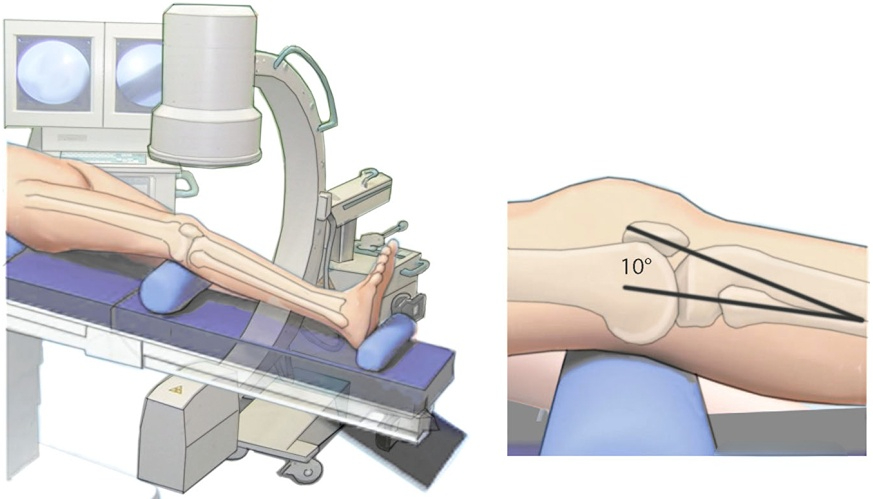
Body position: Supine, knees flexed 10°.
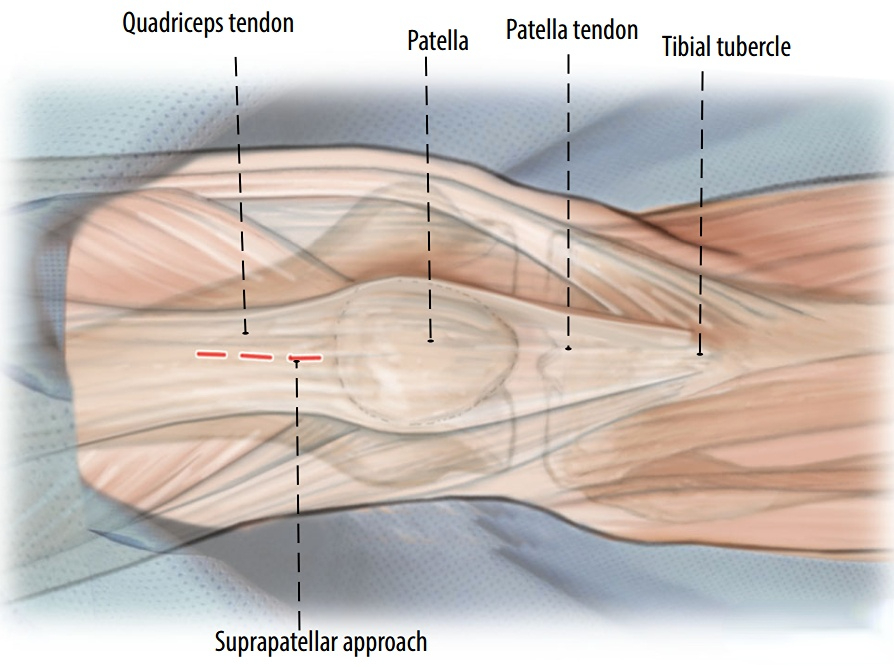
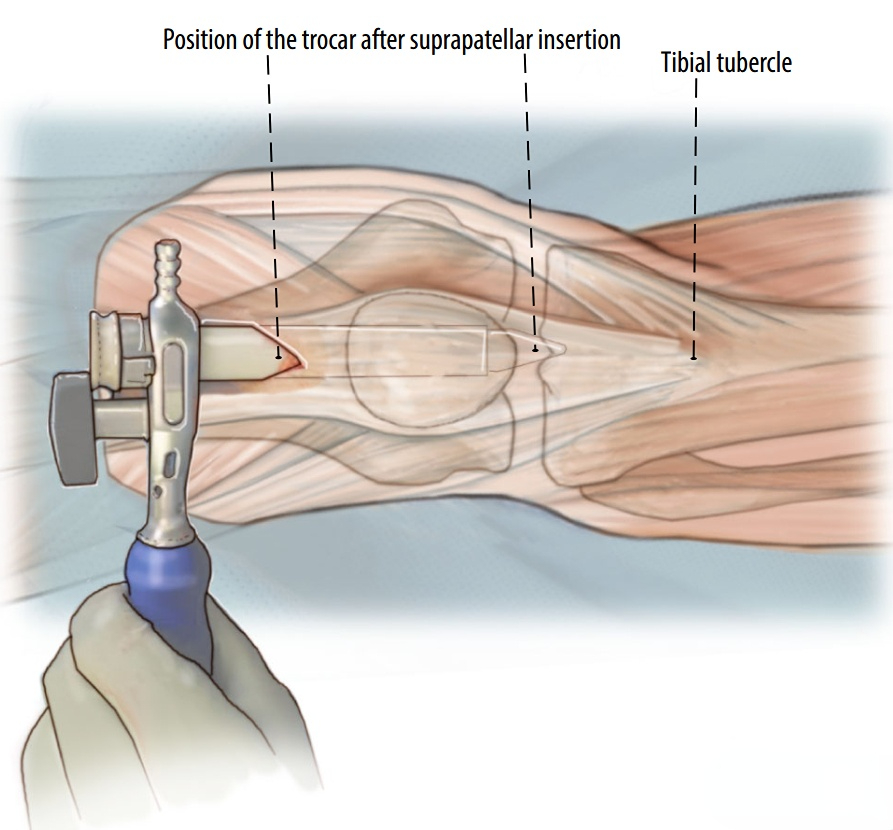
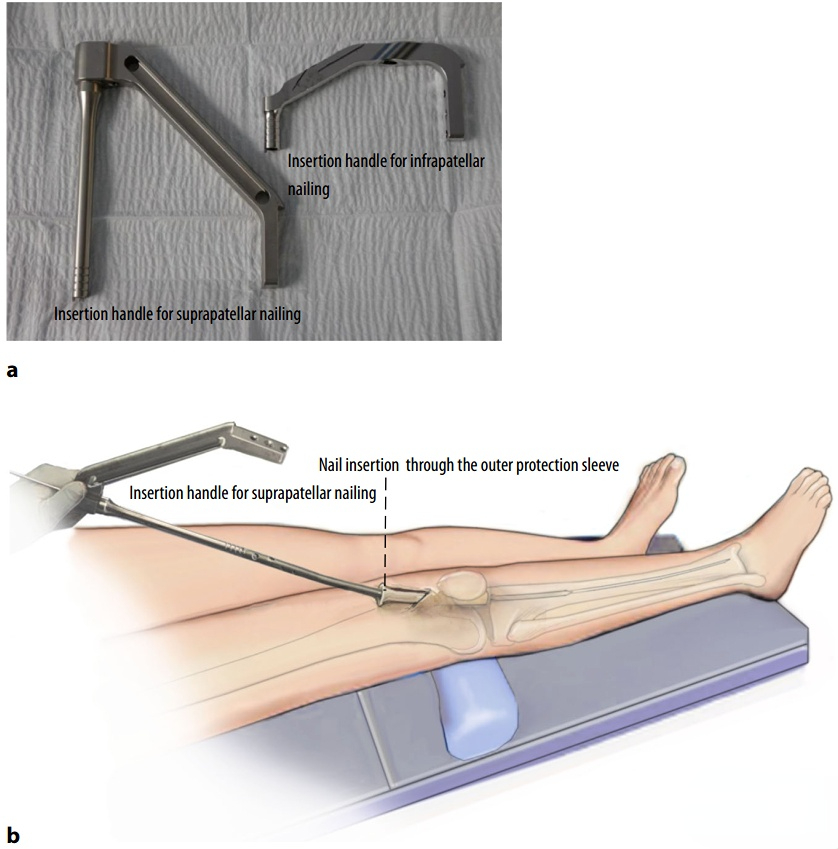
Needle insertion point. Make a 2-cm long longitudinal incision 1.5 cm above the patella along the axis of the patella, tibial tuberosity, and anterior tibial cortex. Split the quadriceps tendon and insert your fingers under the patella to find the needle insertion point. If necessary, elevate the patella.
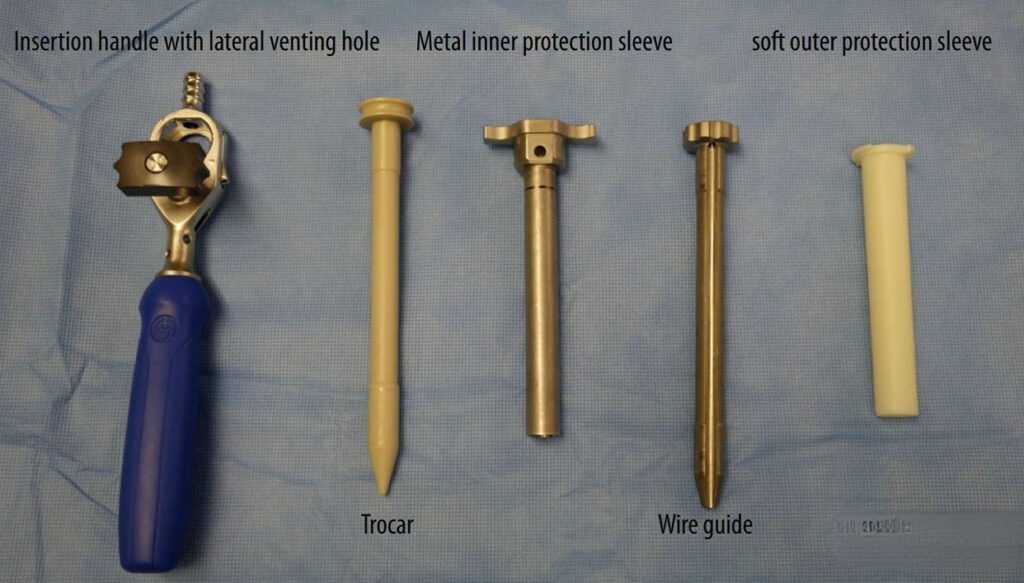
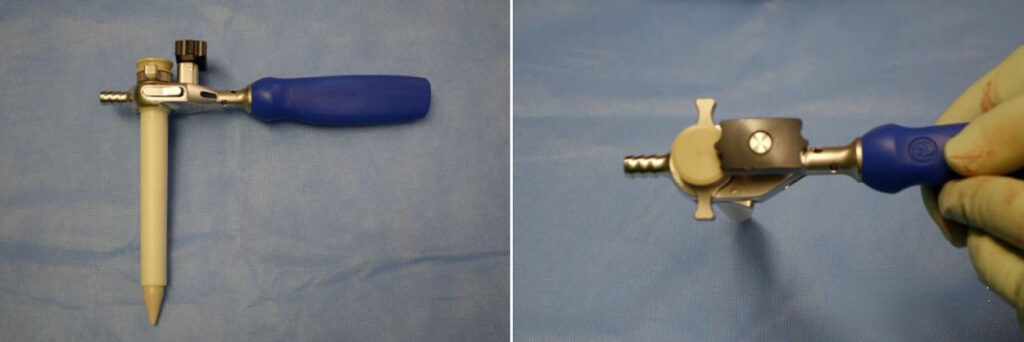
Protection of articular cartilage. A major disadvantage of the suprapatellar approach is that it requires passing through the knee joint and may cause damage to the patella and femoral condylar cartilage, so a sleeve must be used before opening the opening.
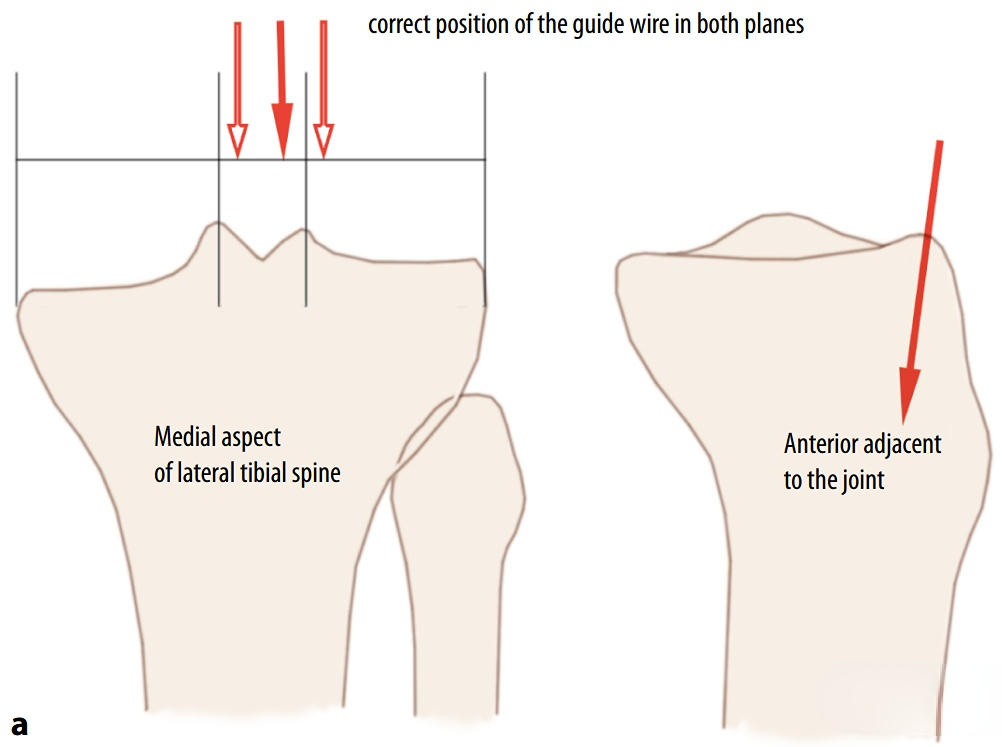
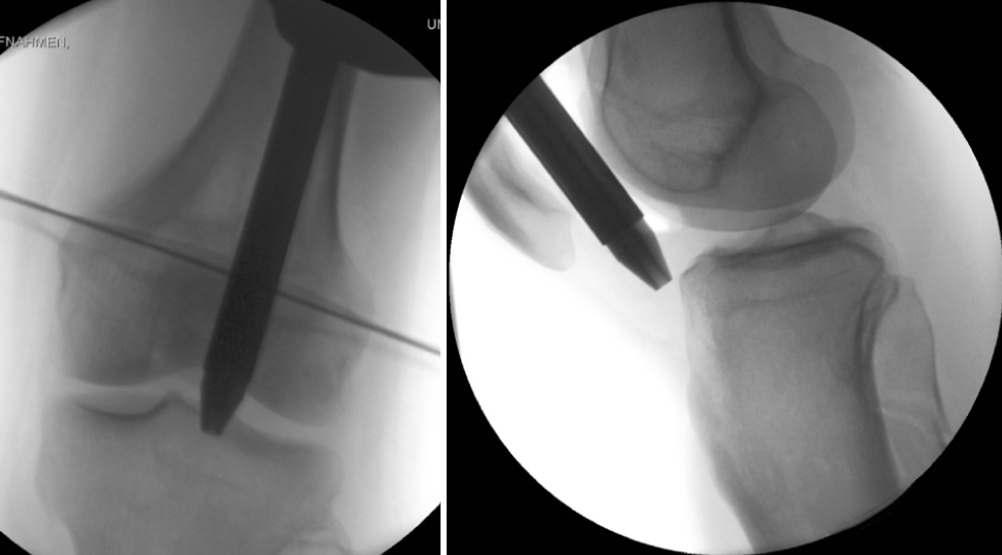
Opening and inserting the guide pin. The ideal position of the guide pin is on the medial side of the lateral ridge of the tibial plateau in the anteroposterior view and at the junction of the plateau and the anterior cortex of the tibia in the lateral view.
Expand the marrow.

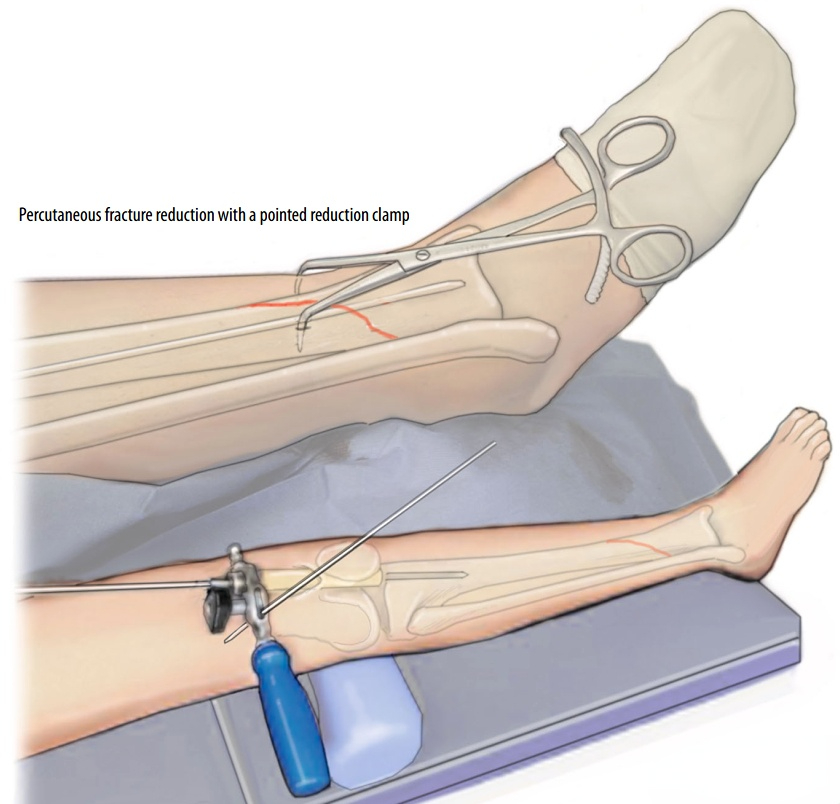
Percutaneous reduction of fractures.
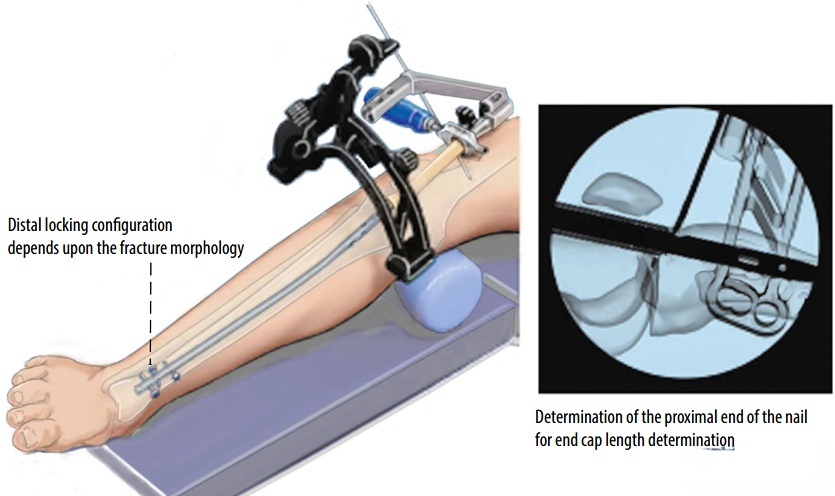
Insert the main nail and interlock the proximal and distal locking nails.
[Statement]: The concepts, technologies, and principles shared on this platform are all publicly available journals, published books, or online platform materials. The copyright belongs to the original author. The platform only organizes, summarizes, and shares them for learning reference. This platform is not responsible for the authenticity of the content or the effectiveness of the technology. The related medical behaviors generated based on the content pushed by this platform have nothing to do with the platform. Please choose carefully.
Welcome to share, forward, and like the article in the lower right corner!