The knee joint is rich in blood vessels and nerves and has a complex bone structure. Exposure and fixation of #tibial plateau #fractures involving the posterior column are still difficult. For tibial plateau posteromedial column fractures, the prone Lobenhoffer approach or the “inverted L-shaped approach” of Professor Luo Congfeng of the Sixth Hospital can be effectively exposed; while for posterolateral tibial plateau fractures, the approach is more diverse, including the Frosch approach and its modification, the Carlson approach, the anterolateral expansion approach, and the fibular head osteotomy approach.
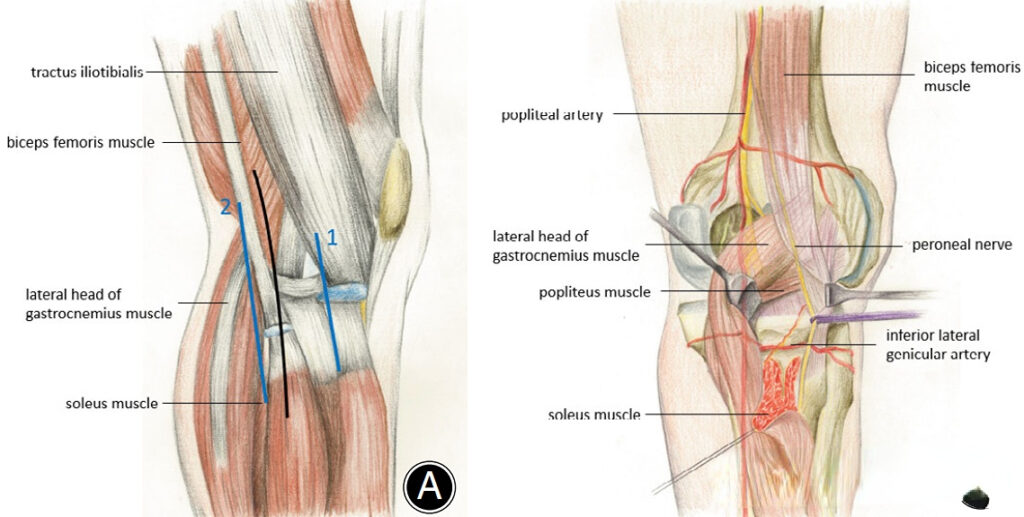
▲ The picture shows the Frosch approach. Line 1 is the anterolateral approach, line 2 is the posterolateral approach, and the black line is the Frosch approach incision.
For tibial plateau fractures involving the posteromedial and posterolateral columns, due to the limitations of the above-mentioned approaches in simultaneous exposure, more scholars use a double incision combined approach for treatment. Double incisions are bound to cause greater trauma, and some surgical approaches may require a change of body position, increasing surgical time and blood loss. To this end, foreign scholars have described a modified oblique Lobenhoffer approach through gross research, which can simultaneously expose the posteromedial and posterolateral columns of the tibial plateau through a single incision in the prone position. This incision can be used alone or in combination with the anterolateral approach. It is introduced as follows:
Surgical exposure steps
Step 1: Separation and exposure of skin incision and subcutaneous tissue.
First, locate the body surface landmarks. Mark the posterior joint line and posterior midline of the knee joint. The skin incision is 1 cm above the intersection of the knee joint line and the posterior midline, and is horizontally and obliquely inward and downward, parallel to the theoretical course of the medial sural cutaneous nerve (to avoid nerve damage).
The separation direction of subcutaneous fat and fascia is the same as the skin incision. Pay attention to retaining some fat and the space between the incision and the medial sural cutaneous nerve.
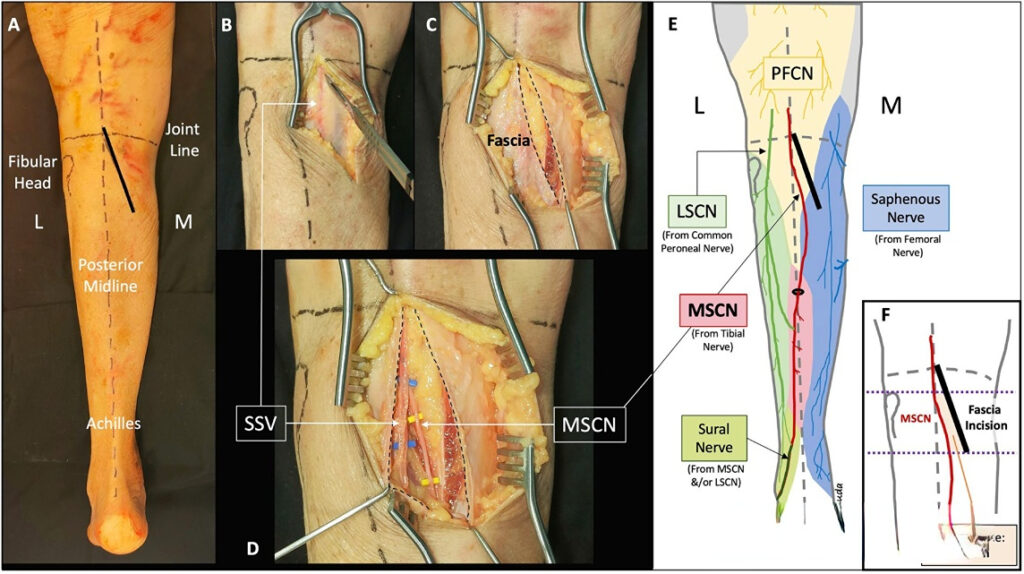
▲ The image shows the separation and exposure of the skin and subcutaneous tissue. SSV: small saphenous vein; MSCN: medial sural cutaneous nerve; L: lateral; M: medial; PFCN: posterior femoral cutaneous nerve.
Step 2: Separation of deep tissues on the posteromedial side.
Pull the medial sural cutaneous nerve and the small saphenous vein outward to expose the gap between the medial head of the gastrocnemius and the pes anserine. After opening the gap, pull the medial head of the gastrocnemius outward to expose the surface fascia of the popliteus and semimembranosus. At this time, bend the knee slightly to relax the medial head of the gastrocnemius.
In this step, there is no need to directly expose the popliteal nerve and vascular bundle. The vascular nerve bundle is located between the gastrocnemius and the popliteus, and normal separation will not damage this structure.
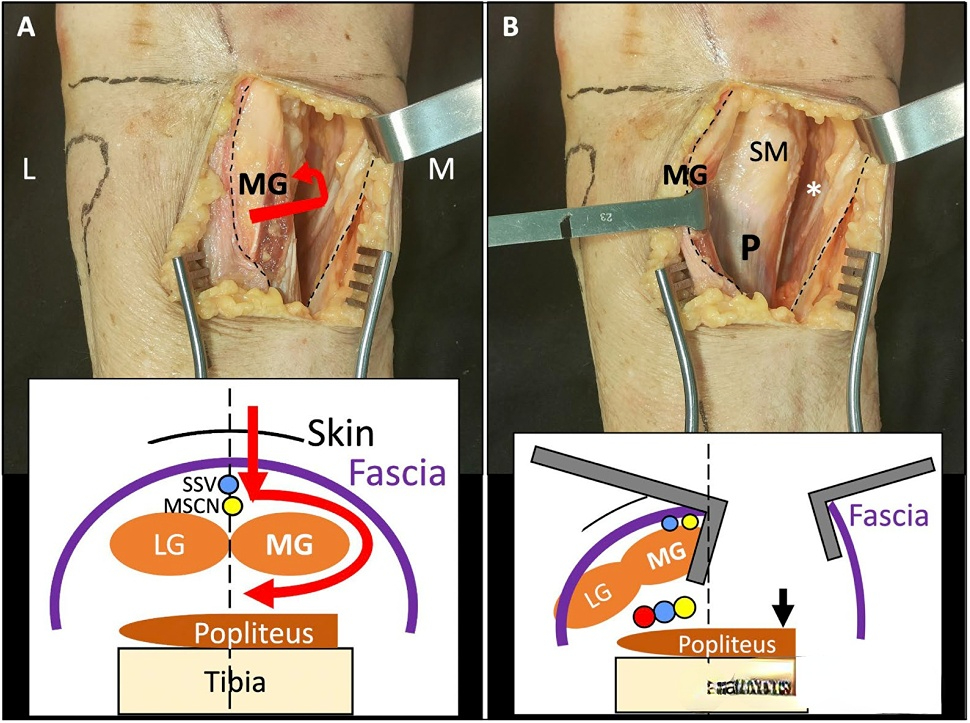
▲ The figure shows the separation of the deep posteromedial tissue. MG: medial head of gastrocnemius, SM: semimembranosus; P: popliteus; LG: lateral head of gastrocnemius; Tibia: tibia.
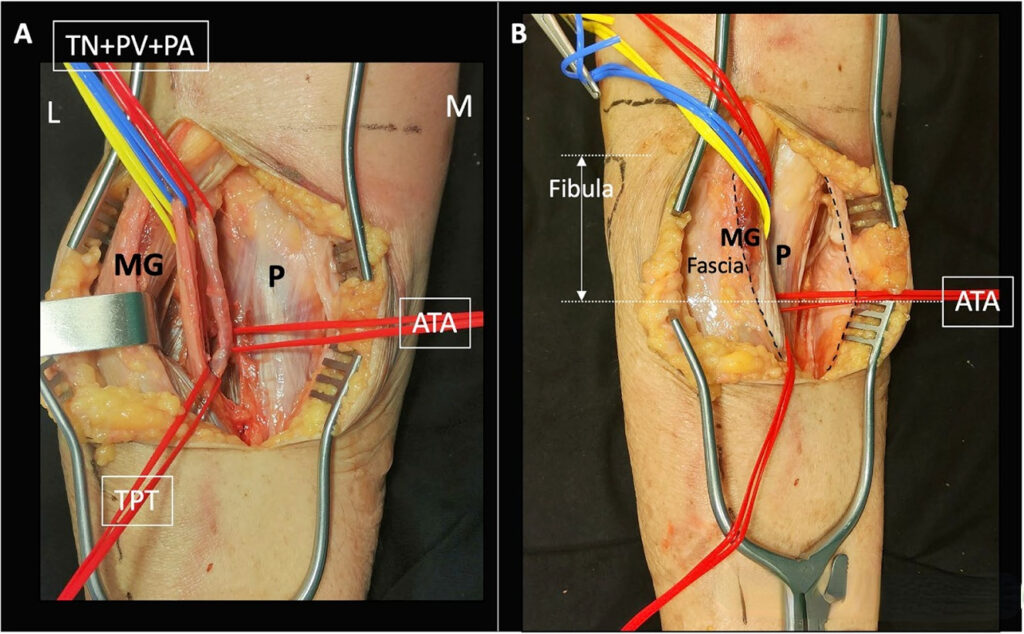
▲ The popliteal neurovascular bundle is shown, but it does not need to be exposed in this approach. TN: tibial nerve; PV: popliteal vein; PA: popliteal artery; ATA: anterior tibial artery.
Step 3: Separate the popliteus muscle and expose the bone surface.
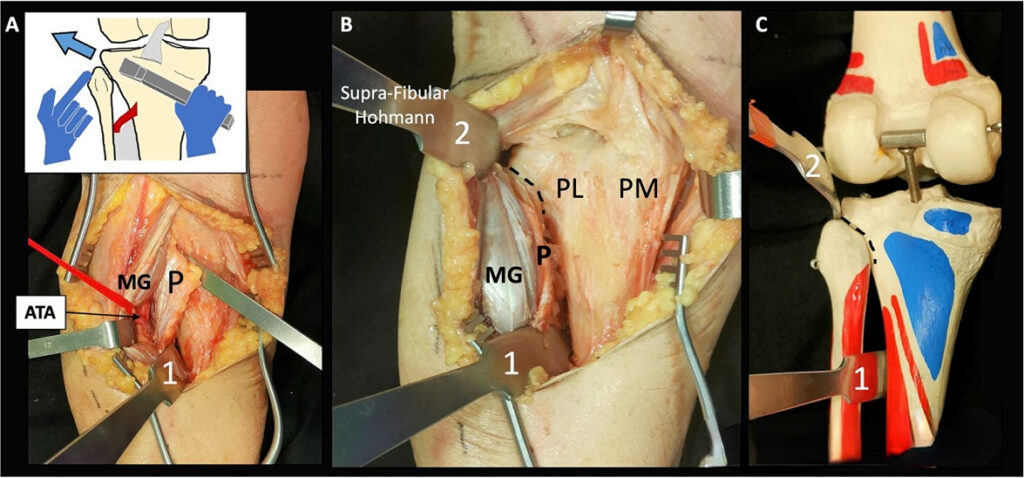
The popliteus muscle and semimembranosus muscle are attached to the posterior medial side of the tibial plateau (blue mark in the figure). After exposing the popliteus muscle, cut from the medial edge of the popliteus muscle. In this step, pay attention to separating and ligating the medial genicular artery. You can cut horizontally between the upper edge of the popliteus muscle and the end point of the capsule machine. The periosteal stripper is separated from the bone surface below the popliteus muscle. At this time, the lateral edge of the posterior tibial shaft can be exposed, and the Hoffman retractor is inserted. Be careful not to damage the anterior tibial artery. Carefully peel off the soft tissue on the lateral side and the fibular head. At this time, the posterolateral platform can be completely exposed, and another Hoffman retractor is inserted from the fibular head.
In this way, the posterolateral and posteromedial columns of the posterior tibia can be completely exposed.
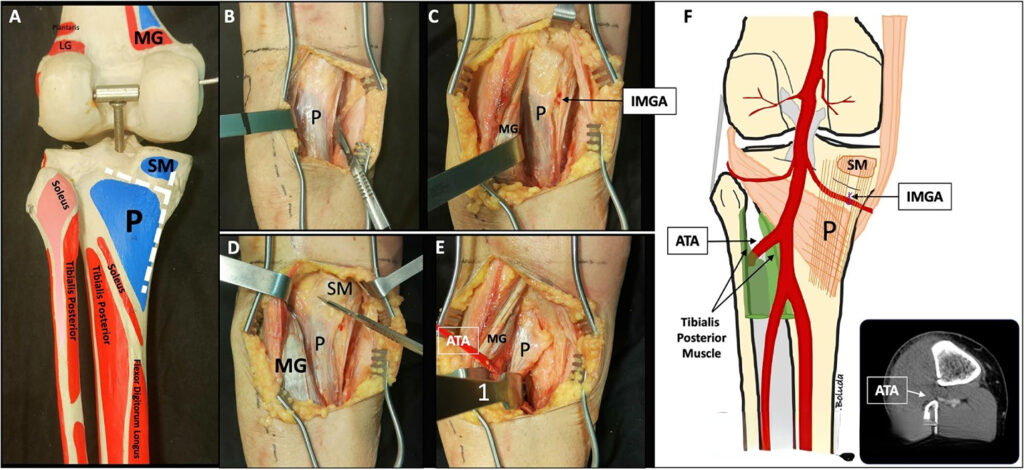
▲ The picture shows the exposure of the posterior tibia. In the blue part of Figure A, P is the attachment of the popliteus muscle, and SM is the attachment of the semimembranosus muscle.
In fractures involving the posterolateral and posteromedial platforms, the bone fragments usually have a certain regular bone displacement direction. As shown in the figure below, the purple is the posteromedial bone fragment, which is usually larger and complete. The posterolateral platform usually has two parts: the posterolateral central bone fragment and the posterolateral lateral bone fragment. The central bone fragment can be displaced downward and is more severely displaced than the lateral bone fragment. The above bone fragments can be effectively reduced through various auxiliary reduction methods.
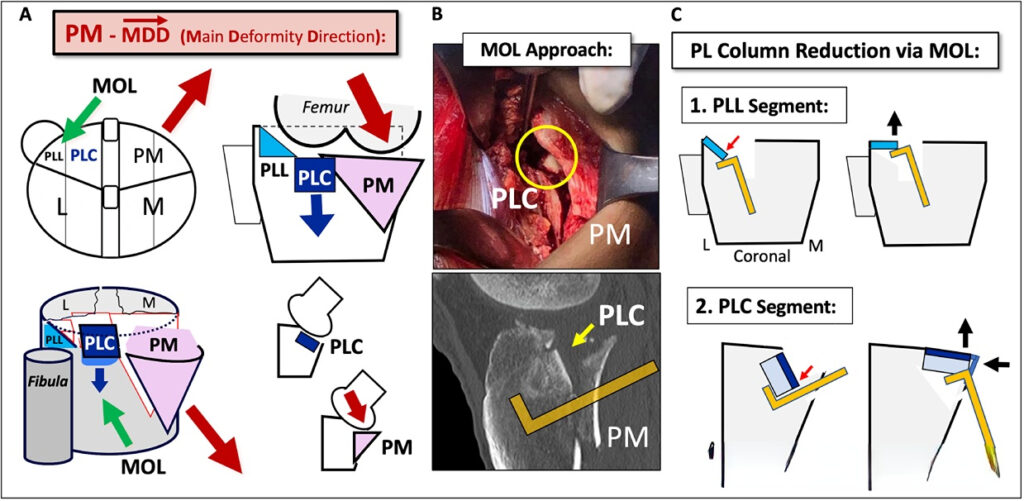
▲The figure shows the general displacement pattern of the posteromedial and posterolateral bone blocks of the tibia.
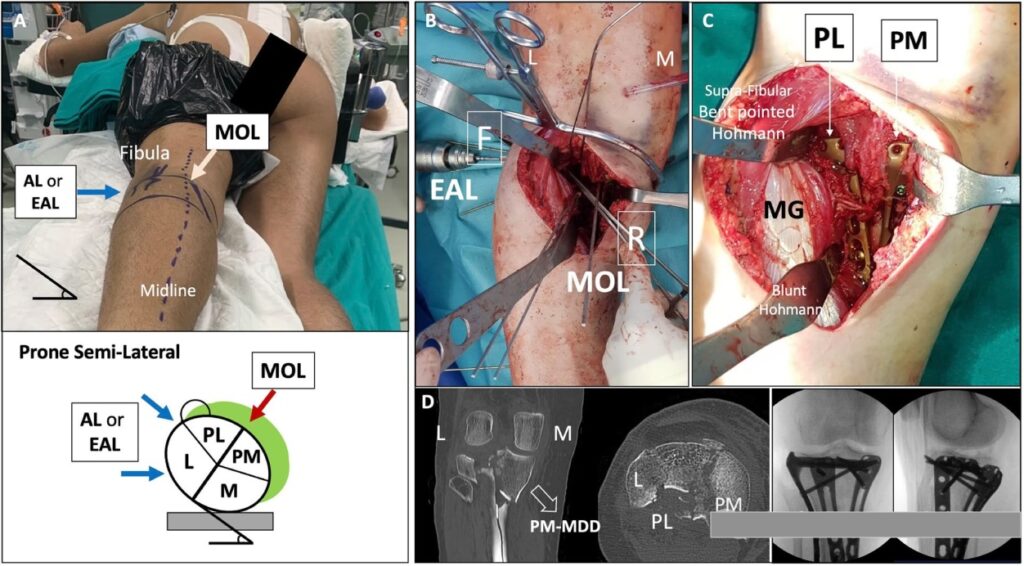
▲ Typical case. This patient was fixed through the MOL approach combined with the anterolateral approach. Figure C shows that the posterolateral and posteromedial plates can be well placed after exposure.
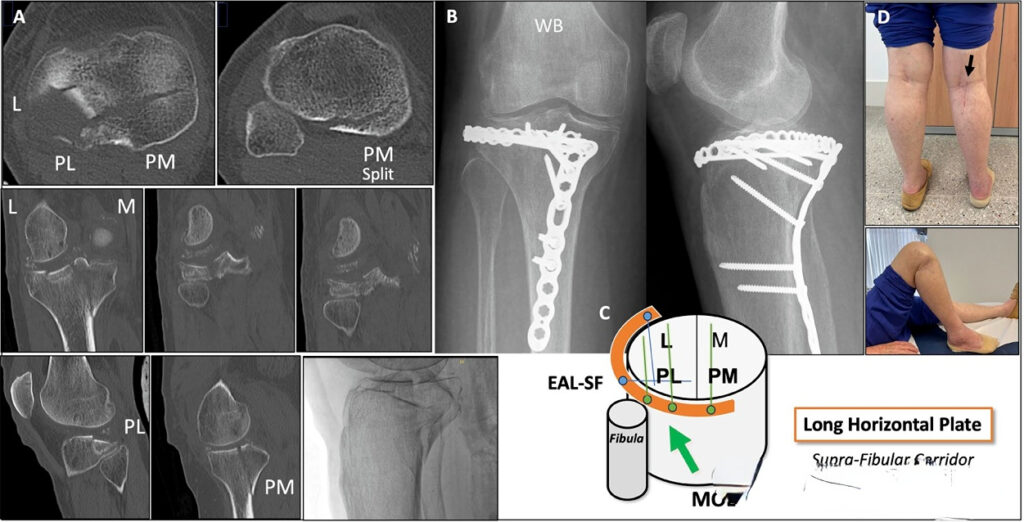
The advantage of this approach is that both the posterolateral and posteromedial platforms are well exposed. The common clinical approach of anterolateral + posteromedial incision can be completed through this MOL approach in most cases. For example, for injuries such as posterolateral platform collapse and posteromedial splitting, the posteromedial support plate + posterolateral horizontal strip plate can be placed through the MOL approach, which usually requires two approaches to complete:
The choice of various approaches is based on the familiarity of the anatomy and the surgeon’s preference. Approaches that can successfully complete the planned surgery are good approaches and can be used as a reference for clinicians.
[Statement]: The concepts, technologies, and principles shared on this platform are all publicly available journals, published books, or online platform materials. The copyright belongs to the original author. The platform only organizes, summarizes, and shares them for learning reference. This platform is not responsible for the authenticity of the content and the effectiveness of the technology. The related medical behaviors generated based on the content pushed by this platform have nothing to do with the platform. Please choose carefully. If there is any infringement, please contact us to delete it.
Welcome to share, forward, and like the article in the lower right corner!