Meta Description:
When should patients begin weight-bearing after tibial plateau fracture surgery? Learn how modern fixation techniques and individualized rehabilitation protocols have redefined recovery timelines.

Understanding the Challenge
Tibial plateau fractures represent one of the most complex injuries around the knee joint. They not only disrupt the articular surface but often involve soft tissue, meniscal, and ligament damage. The decision of when to bear weight after surgery is critical — too early risks displacement or fixation failure; too late risks stiffness, muscle atrophy, and delayed recovery.
There is no universal timeline — the key lies in balancing biomechanical stability, fracture type, and patient-specific factors.
👉 Learn more from the AAOS Tibial Plateau Fracture Guidelines.

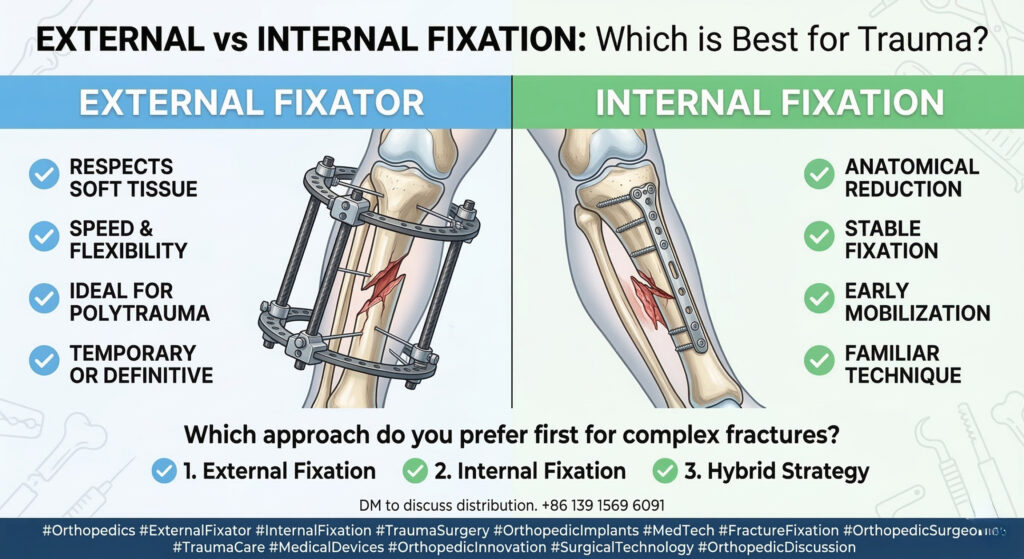
Fracture Classification Determines the Rules
To guide postoperative care, surgeons often rely on Schatzker or AO/OTA classification:
- Simple fractures (Schatzker I–III): usually involve lateral plateau with minimal comminution — more stable and suitable for early partial loading.
- Complex fractures (Schatzker IV–VI): bicondylar or metaphyseal-diaphyseal dissociation — unstable and require delayed progressive loading.
In essence:
“Stable fractures permit controlled freedom. Unstable fractures demand patience.”
The Shift from Delayed to Early Weight-Bearing
Historically, delayed weight-bearing (10–12 weeks post-op) was standard, primarily to protect weak fixation constructs. But modern innovations — like locking compression plates (LCP) and angle-stable screws — changed the game.
Recent meta-analyses covering over 900 patients demonstrated that early weight-bearing (≤6 weeks) does not increase complications.
Key results:
- No increase in pain (VAS score SMD=0.06, P=0.89)
- No increase in delayed union or nonunion rates
- Faster recovery of joint range of motion (ROM)
- Reduced quadriceps atrophy and stiffness
➡️ Early loading, under proper supervision, improves function without compromising fixation stability.
The 3 Dimensions of Weight-Bearing Decisions
Every decision must consider three independent but interconnected factors:
1. Fixation Stability
- Confirm by postoperative X-ray or CT:
- <2 mm joint surface collapse
- No hardware loosening or misalignment
- Modern locking plates allow controlled partial loading early (20–30% body weight).
2. Fracture Type
- Stable simple fractures → start partial loading 1–2 weeks post-op.
- Comminuted bicondylar fractures → wait 4–6 weeks, begin gradual progression with gait training systems or pressure sensors.
3. Patient Profile
- Elderly or osteoporotic: delayed progression, start at 10–20% load.
- Young, healthy, strong fixation: advance earlier under monitoring.
- Diabetic or poor vascular patients: require longer consolidation before load transition.
The Gradual Weight-Bearing Protocol
Regardless of timing, progression must be stepwise:
- Partial Weight-Bearing (PWB): 20–30% body weight for 2–4 weeks.
- Transitional Loading: +10–15% per week, guided by pain, swelling, and radiographic healing.
- Full Weight-Bearing (FWB): achieved at 12–16 weeks if stable healing confirmed.
Paired with:
- Knee ROM training
- Quadriceps strengthening
- Neuromuscular coordination exercises
Early motion prevents scar fibrosis and stiffness, ensuring full return of function.
Why Personalized Rehabilitation Matters
Each patient’s recovery pathway should be as unique as their fracture pattern.
Modern orthopedic rehabilitation rejects one-size-fits-all “time charts.” Instead, it uses individualized, data-driven recovery modeling, combining:
- 3D imaging for mechanical load prediction
- AI-based gait analysis
- Dynamic monitoring of implant stress
This approach ensures precise timing for safe early mobilization.
Clinical Takeaway
The question, “When to start weight-bearing after tibial plateau fracture?” has only one correct answer:
“When fixation is stable, imaging is solid, and your surgeon says go.”
The era of universal delayed loading is over. With today’s locking systems and guided rehab, early controlled weight-bearing isn’t just safe — it’s beneficial.
SEO Keywords
- tibial plateau fracture weight bearing
- early vs delayed weight bearing after tibial plateau fracture
- tibial plateau fracture rehabilitation
- locking plate fixation tibial plateau
- postoperative knee fracture recovery
- bone healing and early mobilization
Disclaimer:
This article and all articles on this website are for reference only by medical professionals; specific medical problems should be treated promptly. To ensure “originality” and improve delivery efficiency, some articles on this website are AI-generated and machine-translated, which may be inappropriate or even wrong. Please refer to the original English text or leave a message if necessary. Copyright belongs to the original author. If your rights are violated, please contact the backstage to delete them. If you have any questions, please leave a message backstage, or leave a message below this article. Thank you!
Like and share, your hands will be left with the fragrance!